Consultation with a doctor Problems associated with tooth loss are growing exponentially. Most of us are missing one or two teeth. According to statistics from the Russian Federation, by the age of 12, 3% of the population loses one or two teeth. By age 17, 12% lose 1 tooth; by age 50, the average person loses 15 teeth. This not only complicates the process of establishing dentition, but also leads to digestive problems, aesthetic defects, and a person begins to feel embarrassed about his smile. Therefore, the number of people who choose implants has increased. But what types of implants are best to get?
Whatever type you choose: fixed or removable dental prosthetics, with us you will achieve the best results.
Requirements for materials for implants
When looking for an answer to the question of what material to make a dental implant from, you should know that this same material must meet several requirements:
- be durable: to withstand chewing pressure (sometimes exceeding 100 kilograms per square centimeter), and also not to destroy the bone with its mass,
- easy to process at the production stage, maintain a given shape throughout its entire service life,
- do not deteriorate (do not corrode) from the action of the biological environment (saliva, blood, etc.),
- do not exhibit toxic, allergenic and carcinogenic effects on the body,
- do not provoke an increase in galvanic currents when interacting with metal structures installed in the patient’s mouth.
These are the basic requirements that can be applied to materials for dental implants - and, of course, every self-respecting manufacturer understands this. As a result, there are not many options left as to what to make a dental implant from.
%akc54%
Implantation methods
The following implantation methods exist:
- Single stage (immediate load)
This technique includes All-On-3, All-On-4 and All-On-6, Basal Complex, zygomatic implantation)
- One-stage (immediately after tooth extraction)
- Two-stage (with delayed loading)
Popular materials for manufacturing
So what material are dental implants made from? All of the above requirements are met by metals and their alloys, as well as oxides of some metals. They are durable and at the same time flexible enough to efficiently redistribute the load without breaking. It is also worth knowing that for the manufacture of implants, for example, plastic, porcelain, glass ceramics or ordinary ceramics are not used (do not include metal-free ceramics, which is called dioxide obtained from zirconium metal!). But these materials are used to create prostheses that are installed on top of implants.
As for medical steel, cobalt-chromium alloy, nickel, gold, they are also not used for the manufacture of implants - but abutments and metal parts of prostheses can be made from them.
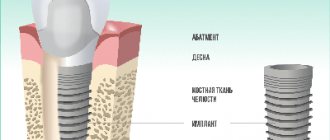
Titanium and its alloys with other metals
When understanding what metal dental implants are made of, you can often find a gray metal called “titanium”. This is not surprising, since it was with this metal that dental implantation began[1]. Since back in 1965, the Swedish scientist Per-Ingvar Brånemark discovered the process of osseointegration - the growth of bone substance on titanium surfaces. That is, it became clear that titanium is bioinert and is completely accepted by the body. Moreover, it is very durable and also lightweight. But not all titanium alloys are used in dentistry and implantology in general. Let's look at which connections are suitable for dental implants:
- titanium alloy of class 4 or Grade 4 according to the ASTM standard: it contains about 99% titanium itself and 0.5% iron. In general, there are 4 classes of commercially pure titanium, which contain virtually no impurities (and those that do exist are harmless). Grades 1, 2, 3 contain much less iron, so they are softer and are therefore not used for implantation. It is worth noting that even pure titanium has a tendency to break down in a humid environment, but manufacturers have found a way out (more on this below),
- Grade 5 or titanium alloy (88%) with aluminum (up to 6.75%) and vanadium (up to 4.5%): Ti-6Al-4V alloy is 3-3.5 times stronger than Grade 4 and cheaper to produce. This high strength makes it indispensable in the manufacture of thin, reliable implants with special compression or aggressive threads, which are installed in the dense basal sections of the jawbone. But the presence of toxic vanadium can slow down osseointegration (engraftment - fusion with the bone).
To prevent commercially pure titanium from being destroyed and vanadium from poisoning living cells, manufacturers came up with the idea of treating the structure in such a way that a dense film of titanium dioxide is formed on its surface. It is bioinert and acts as a kind of barrier. We will tell you in more detail a little later about how the surfaces of implant structures are processed.
The following brands are created from titanium: Nobel Biocare, Straumann, OSSTEM, Oneway Biomed and many others, because titanium is the most popular and studied (about 60 years of observations) material for implantation.
White zirconia
Zirconium is a fairly soft gray metal, but its oxide or dioxide is a super-strong white material that looks like ceramic. Zirconium dioxide can be used to make not only implants, but also between the implant and the crown/prosthesis), as well as crowns. Along with high strength, the material is characterized by a white color - similar to a natural tooth root, which is favorable for the restoration of teeth in the smile area.
The advantages of zirconium dioxide also lie in the fact that it is biocompatible, does not provoke allergies, and is one of the most durable in use. Bacteria weakly attach to the zirconium dioxide surface (adhesion is 40% less than that of metals). Disadvantages - high cost and special processing requirements (milling using CAD/CAM technologies).
What brands use: Straumann (Pure model), CAMLOG.
Roxolid – titanium alloy with zirconium dioxide
This dark gray alloy is a unique and patented development of Straumann. It contains about 15% zirconium dioxide and about 85% titanium. By combining two materials, the manufacturer managed to achieve the highest strength (it is higher than grade 4 titanium). Therefore, implants can be made in smaller sizes, and they will still withstand chewing loads for decades. For example, in the area of chewing teeth, you can place a narrow implant with a diameter of 3.3 mm from Roxolid (although ordinary titanium implants in this area are placed 5-6 mm in diameter). And the system will behave perfectly during operation, will not break under pressure and will be comfortable to wear. The disadvantage of titanium alloy with zirconium dioxide is the high cost of the products.
“Several years ago I had to remove a front tooth, but I didn’t want to put a bridge on. My dentist suggested placing a white zirconium implant and the same crown. What can I say - when I looked in the mirror, I just didn’t understand at first, as if it was my natural tooth that had returned to its place.”
Oksana, review from gidpozubam.ru
Tantalum for trabecular systems
Tantalum, like titanium, is a durable and bioinert metal. However, it is used much less frequently due to the fact that it is not so widespread in the world. Speaking in terms of numbers, titanium is found in the earth's crust almost 3000 times more often than tantalum. Moreover, tantalum is stronger and more refractory than titanium (2-2.5 times), so it is more difficult to process – which ultimately dramatically increases the cost of the material.
Brand: tantalum implants are manufactured by 1 company - the American company Zimmer. Moreover, these are not classical implants, but trabecular ones. The point is that during production, small cells or labyrinths - trabeculae - are formed on their surface. These cells are similar to the own trabeculae of the bone substance (which in the upper spongy layer literally all consists of such cells). This feature has a beneficial effect on osseointegration - the bone grows tightly into the metal trabeculae, reliably holding the implant in place.
Implantation area
How can a patient understand that the implantation went well or complications have begun? The condition is normal when swelling appears after surgery and increases within three hours. After seven to ten days, the swelling subsides. If during this period the swelling does not go away, but increases even more, hyperemia of the skin and purulent discharge appear, then you need to consult a doctor.
The implant may fail several years after the process. Causes:
- patient's health status;
- improper care;
- incorrect installation;
- bad habits;
- doctor errors during surgery.
For the lower jaw, the survival stage is shorter. During the passive implantation process, you need to follow several tips:
- observe the rules of hygiene;
- periodically consult a surgeon;
- carry out antiseptic treatment of tissues;
- take anti-inflammatory drugs;
- follow a diet.
The sutures are removed after 5-7 days, when severe swelling and pain subsides, a temporary prosthesis is put on to reduce the patient’s discomfort. If everything went well, then after 3 - 5 months the pain, bad breath, bleeding gums and discomfort will go away.
Choosing the best material
To determine the best material for a dental implant, you need to take into account not only its quality, but also its availability, cost, versatility - suitability for various clinical situations. If we take into account all of the above, what remains is titanium and its alloys - they can be called the best for implantation. Zirconium dioxide and tantalum have one significant disadvantage - high cost, so they are not available to all patients.
Read on the topic: what is the basis for the popularity of different models of dental implants – and which ones are better.
Although titanium has become somewhat commonplace in implantation, the leader in this field, Nobel Biocare, is in no hurry to come up with something new in terms of material for implants - titanium was, is, and has remained for 60 years. After all, this metal is unique - it is not rare, it is light and exceptionally strong for its mass, it is durable and biocompatible. As for others, in addition to designs from Roxolid, it produces similar models from pure titanium. Oneway Biomed, a developer of basal models that allow implantation in patients with severe periodontitis[2], makes its strongest structures from Grade 5 titanium. But due to contact with the gum and fixation in the stronger layers of the jaw and even cranial bone, they need not so much osseointegration as osteofixation, that is, primary fastening.
Implant selection criteria
Material characteristics are a very important component of the implantation system. But dental implants made from the same material, manufactured by different companies, or even by the same company - but in different “lines”, can be very different. The success of restoration also depends on the following aspects:
- the implant must be standard, manufactured at a factory: production is carried out using milling, intense plastic deformation (a rarer type). Individual structures made in a regular dental laboratory are not recommended for installation, because their service life is short (about 7 years),
- shape of the structure: now the best are considered to be root-shaped and cylindrical,
- type of thread: it can be sharp with the ability to self-cut, it can be compression - compact the bone tissue around itself,
- surface: it can be smooth and polished by a laser, or rough - processed in an electrolyte solution or using sandblasting. Active substances that stimulate the growth and restoration of bone tissue cells - fluorine, calcium, phosphorus and others - are also applied to the surface.
- sterilization: modern technologies at the production stage allow for 5-stage treatment to remove impurities,
- a correctly selected model for a specific clinical case: therefore, before implantation, patients undergo tests and undergo a computed tomography scan of the jaw. This way, the doctor can identify important features (for example, changes in hormone levels, the presence of inflammation, atrophy of the jaw bone) and choose an implant based on the indications. And in his choice he is helped by 3D planning in a computer program, for example, Simplant, NobelClinician,
- a good implantologist: this item can be put at the top of the list, because the success of implantation depends on the professionalism of the doctor and his responsible approach to the matter.
What is transocclusal (screw) fixation?
When attaching a crown to an implant, two types of fixation of a dental crown to an implant are used: screw and cement.
Screw fixation can be implemented in two ways. The first is that the abutment is permanently connected to the crown, the structure is inserted into the implant and fastened to it with a screw (a through hole for the screw is first made in the crown). The second is that the abutment is installed on the implant, the crown is installed on the abutment and attached to it with a screw. The hole in the crown is called a tunnel; it is closed with a tooth-colored filling.
When using screw fixation, the technician will require higher qualifications, because... even small deviations from the size will not allow you to install a crown in your bite
Cement fixation . First, the abutment is screwed to the implant, and then the crown is fixed with cement mortar (composite adhesive) with shock-absorbing properties - just like a regular crown on the tooth stump.
The screw type of fixation is more reliable, convenient and safe. If you need to fix something, you can drill out a filling on the tooth, unscrew the screw and remove the crown. This allows you to save the rest of the structure, correct the mistake and place the crown again.
Cement fixation is used when installing bridges on two or more implants. In this case, high precision must be observed (in order to attach the bridge to the required number of implants). This method of fixation “forgives” the errors of the dentist and technician, but it will be difficult to remove the prosthesis later. Recently, advanced technologies have been used in dentistry, and installation errors occur only due to the low qualifications of the doctor or violation of established standards. Therefore, cement fixation of prostheses is used less and less.