Clasp dentures, popular in prosthetics, are not a new technology at all. The first development was proposed by a German doctor at the beginning of the last century. Hence the name. Bugel means “arc” in German.
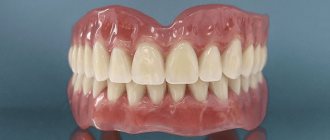
This type of prosthesis is distinguished by its strength, reliability and durability. The design includes an arch on which artificial teeth are attached, a saddle (bridle), a base and a mount for supporting teeth. This structure ensures reliable fixation of the product in the oral cavity. Used to restore teeth with partial edentia.
In addition to reliability, the clasp denture preserves the functionality of the dentition and evenly distributes the load on the jaw. The design has a high level of aesthetics and does not cause discomfort when worn. The absence of a bulky base saves the patient from constant cleaning of the product. In addition, the prosthesis does not need to be removed at night. Let's talk about the nuances and types of products.
Classification
Clasp structures refer to a removable or conditionally removable method of prosthetics. They are divided by type of material and type of fastening. The base of the prosthesis, the arch, is made of three types of material:
- Made from medical alloy (cobalt, chromium).
- Noble metals (gold-platinum).
- Plastics.
It is obvious that metal-free clasp dentures are less durable, wear out quickly and break under load. However, it is an inexpensive alternative for patients with high sensitivities and metal allergies.
A more durable option is made from an alloy of gold and platinum. Also suitable for patients with allergies, but costs several times more.
Types of clasp dentures
Clasp structures are a solid frame made of metal (cobalt-chromium alloy), onto which a retaining arch, a base made of acrylic material and a base with artificial teeth are attached.
Supporting and retaining elements can be:
- solid;
- composite (metal elements soldered together);
- separate (wire elements subsequently soldered together).
In addition, clasp structures can be attached to the patient’s jaws in different ways. Such mounting options can be:
- metal clasps (or hooks);
- locks (attachments);
- telescopic system.
Let's try to evaluate the most important advantages and disadvantages of various types of fastening these removable dental plates.
Mounting type
Fixation of clasp dentures is carried out due to the patient’s neighboring (healthy) teeth, which are used as a support. The structure can be fixed:
- Using locks. The upper part of the lock is placed inside the artificial teeth, and the lower part is in a metal crown, which is installed on the supporting teeth. This provides additional protection and reliability to your own teeth. And evenly distributes the load on the supporting teeth. Externally, the prosthesis looks very neat and aesthetically pleasing. And it can be easily removed if necessary. The disadvantage of the product is its high cost due to the use of additional materials.
- Hooks (clasps). The most affordable and simple fixation system. The hook grips the abutment tooth. The cast design and metal clasp guarantee high-quality fasteners and a tight fit to the tooth. Each hook is produced in accordance with the size, shape and anatomical features of the abutment tooth. Therefore, accidental loss of the structure from the mouth is excluded. The downside is that the hooks may be visible in the mouth. For example, when talking or eating.
- The third type of fixation is telescopic crowns. In this case, two crowns are used. The first is installed on the supporting dental unit. The second is inside the prosthesis. The size of both crowns is calculated so that the outer one fits tightly onto the inner one.
The last type of fastener is considered the most optimal. Even if the supporting tooth is destroyed, the inner crown will hold the denture. The adjustment will be minor. However, the development of a clasp prosthesis with telescopic fixation requires highly qualified specialists. Both a doctor and a dental technician.
Clasp system - Clasp denture with clasps
The clasp system is the most common system for fixing and stabilizing a clasp prosthesis. In a clasp denture, the clasp is support-retaining, which means that the tooth not only serves to keep the denture from moving, but also absorbs part of the chewing load falling on the denture.
The many types of clasps led to the need to systematize them, therefore, in the first half of the last century, the Ney clasp system was developed in the USA, which combined 5 types of clasps.
Ney's clasp system
Type I clasp – Acker clasp
On the Acker clasp, it is most convenient to consider the device and the function of the clasps in principle.
The clasp has three parts:
- a shoulder adjacent to the tooth and performing a supporting and retaining function;
-an occlusal pad, which is located on the occlusal surface of the tooth and transfers part of the chewing pressure to the supporting tooth;
-body - the area where the shoulder and the occlusal pad of the clasp meet;
- a process connecting the clasp to the frame of the clasp prosthesis.
The anatomical shape of the teeth provides for the presence of an equator, which, if necessary, can also be recreated with prosthetics. So, the equator divides the tooth into two parts: the gingival part, located between the edge of the gum and the equator of the tooth, which is also called retention or retaining, and the supporting part, located above the equator to the occlusal surface of the tooth. As we remember, the clasp shoulder in a lamellar prosthesis was located under the equator of the tooth, so the clasp performed only a retaining function (being located in the retaining zone), but the clasp in a clasp is more complicated. The shoulder of the clasp “hugs” the tooth, located simultaneously in the retaining (retaining part of the shoulder) and support zones (stabilizing part of the shoulder), which is why it performs a support-retaining function and is called accordingly. The retaining part of the shoulder is not capable of transmitting chewing pressure to the supporting tooth, therefore it participates only in the retention of the prosthesis and resists displacement of the prosthesis in the occlusal direction. The stabilizing part of the shoulder “lies” on the surface of the tooth, which prevents the prosthesis from sagging towards the gum.
Thanks to its elastic properties, the clasp arm is able to overcome an obstacle in the form of the equator and enter the holding zone. But sometimes this elasticity becomes insufficient, so a second type of clasp comes to the rescue.
Type II clasp – Roach clasp
Unlike the Acker clasp, the shoulder in the Roach clasp, moving away from the body, is directed first to the gum, where, after a semicircular bend, it moves towards the retention zone and ends in a T-shaped branch. This shape of the shoulder makes it longer and, as a result, less rigid than the shoulder in the Acker clasp. This form makes it possible to achieve the location of the retaining part of the shoulder in a tooth with a small area of the retention zone, or in teeth when the close location of the equator to the occlusal surface does not leave room for the stabilizing part of the Acker clasp. Also, the Roach clasp is more aesthetically pleasing compared to the previous one, since most of the shoulder is moved from the surface of the tooth.
But Roach's clasp is not without its drawbacks. This is the weak stabilizing effect due to the weak coverage of the supporting part of the tooth and less rigid shoulders, which is partially compensated by the larger area of the occlusal lining. Also, pronounced bony protrusions can interfere with the shoulder of the clasp located above the gum, and its less rigidity can lead to its bending if the prosthesis is handled carelessly.
III type of clasp - combined Acker and Roach clasp
With a pronounced inclination of the tooth, it can be observed that one surface is suitable for an Acker clasp; favors the location of the Acker clasp. The strongly pronounced equator on the side of the Roach clasp gives it even more holding properties. On the opposite side of the Acker clasp, the equator approaches the gum, which increases the area of the support zone and the degree of corresponding action of the clasp. Thus, the lack of either supporting or retaining function is compensated, making this clasp design the most favorable for pronounced inclination of the chewing teeth.
Type IV clasp – rear-acting clasp
When molars are lost, the premolars, which are used as supporting teeth, are subjected to enormous stress, so the likelihood of their dislocation increases. However, the design of the rear-action clasp makes it possible to redistribute the application of forces, mainly to the mesial zone of the occlusal surface of the crown. In this case, the tooth will not dislocate from the socket, but rather move into the socket along a path close to the longitudinal axis of the tooth.
The design that allows for such application of forces is one arm, starting from the body and covering the oral, mesial and vestibular surfaces of the crown with the occlusal lining located on the mesial side of the occlusal surface of the tooth. On the oral side, the shoulder does not cross the equator of the tooth, therefore, in this place it serves as a stabilizing part of the shoulder. The retention part is the part of the shoulder that, on the vestibular side, is located under the boundary line and prevents the prosthesis from moving in the occlusal direction.
From this design it follows that the stabilizing part of the shoulder significantly prevails in length over the retention part, which means that the stabilization of the prosthesis will be weakened. Therefore, this clasp design has found its greatest application on premolars with a subsequent end defect on the lower jaw, where retention of the prosthesis is not as important as on the upper jaw.
V type of clasp – ring clasp
The ring clasp is designed for single-standing molars, can have one or two occlusal pads and has design features for molars of the upper or lower jaw.
Any single teeth used as a support have an increased and very real risk of being dislocated, which is why it is important to correctly distribute the load on them to minimize the predominance of the load on one side, and, as a result, the threat of dislocation. This can be achieved by distributing areas of application of forces along the perimeter of the tooth due to one covering arm and two occlusal pads - mesial and distal.
This clasp starts with the shoulder on the side of the defect, but the further course of the shoulder is different, depending on whether the molar belongs to the upper or lower jaws. The molars of the upper jaw have a more pronounced inclination in the vestibular side, that is, they diverge, while the molars of the lower jaw tend to converge, that is, have a lingual inclination. As a result, there is a connection between the inclination and the location of the retention and stabilizing part of the shoulder, similar to the combined Acker and Roach clasp discussed above. On the molars of the upper jaw, the stabilizing part of the shoulder is located on the palatal surface, covers the approximal surface, where it can have an “outgrowth” in the form of an occlusal lining and passes into the retention part of the shoulder on the vestibular side. The clasp for mandibular molars has the opposite design - it begins with a stabilizing part on the vestibular surface and ends with a retention part on the lingual surface.
Ney's system does not cover all types of clasps. There are many modifications of clasps from the Ney system, and completely different designs, however, with the help of the description of the Ney system, an idea of the essence of clasps as a whole is formed.
pros
Unlike soft removable dentures, arch structures do not rub the gums and do not cause long-term addiction. Due to the tight fixation, the mobility of the product in the mouth is eliminated. The structure of the prosthesis does not block the palate - this preserves taste sensations during meals. In addition, the clasp denture does not block the movement of the tongue in the mouth. This does not distort diction and does not cause spasms of the facial muscles.
The distribution of load during chewing of food occurs according to the “one to two” principle. That is, one-third of the pressure is on the support unit and two-thirds on the beam system. The arc takes away part of the load, which protects soft tissues from damage and deformation. In classic removable dentures, the chewing load is directed to the gums and palate.
The structural features of the clasp prosthesis determine its shelf life. With proper care, the product will last at least 7 years, while soft prostheses provide functionality for up to 5-6 years. In the absence of a frame in soft removable dentures, the prosthetic bed quickly collapses.
Another advantage of the design is the possibility of parallel dental treatment with a prosthesis installed. Such products are called splinting - they simultaneously replace missing teeth and tightly fix existing ones.
Caring for a clasp denture
As already mentioned, the clasp prosthesis does not need to be removed at night. You can wash it in the morning after sleeping and in the evening after eating using a toothbrush. There are many products for caring for dentures, including rinses. The doctor can explain to you how they work and help you choose based on the materials of the clasp prosthesis.
Clasp dentures are not suitable for everyone. The condition of the teeth is important, as well as the general reaction to the materials from which the prosthesis is made. However, here too experts have found a way out, using a special type of plastic that does not cause allergies. The cost of such a clasp prosthesis will be a couple of thousand rubles more than a simple one, but you will be able to use it with great pleasure.
No patient can choose a denture option on their own. Only the dentist will determine the condition of the jaw and supporting teeth, and also select the type of clasp denture.
All you have to do is make an appointment with a dentist at our center and receive all the comprehensive information from him. Once you understand what a clasp prosthesis is, we are confident that you will give us a positive review, like many others.
Minuses
The choice of material and fastening can affect the price of the orthopedic structure. The cost can increase 2-3 times compared to analogues.
For metal clasp dentures, there remains a risk of allergies. In addition, the prosthesis cannot be used to restore the entire dentition. To fix the prosthesis, healthy supporting teeth are needed. An alternative is to install implants as support units.
The risk of receiving a low-quality product in the case of arc structures is also very high. You need to carefully choose specialists and a dental clinic for prosthetics.
If there are no outer teeth in the row, the process of fixing the prosthesis becomes more complicated. The structure only needs to be secured on one side. The locking method of fastening ensures good stability of the clasp denture in the mouth. However, the risk of spontaneous displacement still remains (end defect).
Varieties
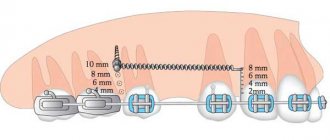
With rectangular profile
The rectangular beam, which became widespread, was first invented by K. Rumpel. Its peculiarity is that the main pressure is transferred to the beam and only a small part falls on the mucous membrane of the alveolar process. There is a gap of 1–2 mm between the bar and the gum to perform hygienic procedures.
With an ovoid profile
The beam structure, developed by E. Dolder, has an ovoid profile with a height of 3 mm and a width of 2 mm. A metal strip 0.2 mm thick acts as a bushing. The gap between the middle of the bushing and the highest point of the beam is 1 mm. As chewing load increases, the sleeve moves, thereby improving the functionality and performance of the system.
With T-profile
Research conducted by Selchukov S.G. allowed us to come to the conclusion that the T-shaped profile has the least deflection compared to other structures. The beam made of cobalt-chrome-nickel alloy is attached to push-button cylindrical locks and is equipped with platforms along the entire length. The matrix is made of polypropylene. In order to improve the shock-absorbing and fixing properties of the system, a gap of 1 mm is left between the upper part of the beam and the matrix. Push-button locks provide reliable adhesion to the supporting teeth, which generally has a positive effect on the strength of the structure.
With cast blanks
The first use of cast blanks for a beam-type prosthesis was proposed by RT Williamson in 1991. Their installation required preliminary processing of the remaining teeth. Its goal was to obtain smooth surfaces without sharp corners and an occlusal gap for fixation of artificial units.
Then plastic pins are inserted into the previously prepared root canals for the subsequent production of their metal counterparts. The cavities into which the pins will be installed are covered with cotton balls and a bandage, which eliminates the risk of infection. Based on the impressions obtained, metal pins are cast, which, after polishing, are fixed to the patient. If necessary, correction is carried out, and then a prosthesis is made by a specialist in a dental laboratory. After polymerization of the plastic base, the prosthesis is ground and polished. Replacement clamps are then installed. This technique significantly reduces the cost of prosthetics, and also improves the fixation of the structure and the condition of the periodontium by shortening the crown.
Contraindications
Clasp structures are not used in cases of complete edentia and the absence of outer teeth in a row. The presence of inflammation in the root canals of supporting teeth may delay the installation of a clasp denture for treatment. If the inflammation is not eliminated, it can lead to tooth loss. And, as a result, to replacing the prosthesis.
Limitations for installing a prosthesis also include incorrect bite, severe abrasion of the enamel, and allergies to the materials used.
For high-quality fixation of the structure in the oral cavity there must be at least 6 healthy teeth in the upper and lower jaw. Otherwise, you will have to choose another prosthesis or supplement the series with implants.
Clasp dentures have a number of advantages over bridges:
- Installation of clasp removable dentures does not require preparation of some teeth and does not limit their mobility.
- Chewing pressure is evenly distributed between the alveolar processes and the remaining teeth.
- Clasp dentures are hygienic; they can be cleaned mechanically outside the oral cavity.
To individually assess the condition of your teeth and make various solutions to your problem, you need to have a free consultation with an orthopedic dentist. A highly qualified specialist will help in any of your situations.
Design development
Like most types of prosthetics, the manufacture of a clasp prosthesis consists of two stages: preparation for installation and production of the structure.
It all starts with a thorough diagnosis of the patient’s jaw. The initial examination is complemented by an x-ray examination, which determines the condition of the teeth and root canals. It also shows the presence of pathologies in both jaws. In more complex cases, EspaDent clinic specialists use a modern 3D tomograph with layer-by-layer images of the jaw. During the diagnosis, the doctor also checks for allergic reactions to the materials used. Based on the clinical situation, wishes and capabilities of the patient, the dentist selects a suitable prosthesis.
The preparatory stage for installing a clasp prosthesis includes:
- Sanitation (cleaning) of the oral cavity.
- Elimination of carious cavities and inflammatory processes in supporting teeth.
- Grinding of teeth and fixation of crowns (for locking and telescopic structures).
Treatment of supporting teeth can cause discomfort, so the procedure is carried out using local anesthesia - safe and painless.
In order for the dental technician to begin making the partial denture, the doctor takes impressions of the prepared jaw. Then follows the calculation part, on the basis of which the specialist creates a wax model of the clasp. The sample is used to produce a metal arch onto which a temporary base and new teeth are installed.
The intermediate product is given for fitting. The patient evaluates the convenience of the design, the reliability of fixation in the oral cavity, and the level of comfort when moving the jaw. If necessary, the prosthesis is adjusted and then the final version is made. In the production of the base, artificial gum, plastic or nylon is used.
After installation, the doctor gives recommendations on how to care for the product. The process takes 3-4 weeks. The time frame may extend due to the need for preliminary dental treatment.
Design nuances for both jaws
The structure of the prosthesis depends on the installation site. For example, a clasp denture is installed on the upper jaw using locks and clasps (hooks). The first method is more popular because... In addition to fixation, the locks provide high-quality support during chewing loads. The hidden fastening mechanism of lock-type prostheses ensures high aesthetics and does not interfere with eating.
Indications for installing a prosthesis on the upper row is the impossibility of implantation. And also the so-called “flat palate” syndrome - atrophy of the alveolar processes.
Unlike the upper row, the clasp denture on the lower jaw can be attached in any of the available ways. The difference between the designs is the location of the arc and fixing elements. In an upper denture, the arch may be located in front or in the middle of the palate. There is also a difference in the shape of the arc: in the form of a jumper, a ring or a crescent.
Locking fastenings - Clasp prosthesis on attachments
In addition to clasps, locking connections, or attachments, are capable of holding a tooth and transmitting chewing pressure to it. Despite the difficulties that can arise when using attachments in the construction of partial dentures, they are an excellent replacement, and quite often an element of choice, given their positive aspects.
So, attachments are small locking fasteners, the connection of which is ensured by a matrix on one side and a corresponding patrix on the other. This is where the first difference between attachments lies - they can be intradental, when the locking fasteners are connected inside the volume of the tooth, or extradental, when the elements are connected outside the tooth. Intradental connections are more physiological in relation to the periodontium of the tooth, since the dislocation force is minimal, however, the production of such a structure requires a larger volume of preparation of the hard tissues of the tooth, and sometimes depulpation of the tooth. If it is necessary to depulpate a tooth, or rather its pulp, an extradental locking connection will be more physiological, however, the point of application of forces is located at a greater distance from the longitudinal axis of the tooth, which is why the dislocation forces are greater than in the first option. The extradental connection will have a beneficial effect on the integrity of the tooth due to the preservation of buttresses that protect the tooth from fracture and internal redistribution of pressure, however, the dislocation moment will gradually adversely affect the periodontium of the supporting tooth.
Another difference between locking fastenings is their mobility, different degrees of which are used for different topography of defects and the condition of the periodontium of the supporting teeth. For example, for defects of Kennedy class I and II (Bilateral and unilateral end, respectively) or if there is a fear of progression of destructive changes in the periodontium, the use of movable locking joints is justified: rotary or hinged. When defects are included (Kennedy classes III and IV) and the periodontium of the supporting teeth is strong, fixed locking connections are used.
Among the positive qualities of attachments, their invisibility is important, and as a result, the aesthetics of dentures in the oral cavity. Locking fastenings make it possible to classify clasp dentures as semi-physiological due to the fact that part of the chewing pressure is transferred to the periodontium of the supporting teeth and they do this successfully, on par with clasps. In addition, the locking fastening as an engineering structure is more complex, since it requires tooth preparation, and sometimes significant preparation. They are also picky about both the clinical height of the crowns and their buccolingual dimensions, which is why the use of attachments may be limited when the teeth are worn and the crown height is reduced to less than 5-6 mm and in the anterior group of teeth, where the buccolingual dimensions are smaller than those of chewing teeth.
As mentioned above, the use of locking fasteners requires preparation of the supporting teeth, and the disadvantage is not only the fact of damage to the hard tissues of the tooth, but also their further covering with special crowns, which is an additional cost for the patient, given that the crowns must also be aesthetic, so as not to lose one of the advantages of the clasp denture design using locking fasteners - their appearance.
Care Tips
Any orthopedic structure will last longer if it is properly cared for. General recommendations for clasp dentures are simple:
- Clean your dentures regularly and thoroughly with a toothbrush.
- Rinse the structure after eating food.
- Periodically remove and soak the product in a special solution. Each structure has its own frequency at which the structure can be removed so as not to damage it. The doctor tells the patient about the peculiarities of care after installing the clasp prosthesis.
To avoid damaging the surface of the crowns, it is not recommended to use whitening pastes or too hard toothbrushes. It is also important to visit the dentist 1-2 times a year for preventive procedures.
Price
The price for this very popular type of removable dentures has a fairly wide range. The cost of structures is influenced by the following factors:
- degree of complexity of preliminary dental treatment before prosthetics (dental treatment, removal, plaque removal);
- production of prosthesis and its installation;
- type of fasteners.
The price in Russia of clasp prostheses with clasps of a simple design starts from 15,000 rubles, and the cost of a splinting or complex clasp prosthesis starts from 20,000 rubles.
The price of clasp structures with micro-locks is an order of magnitude higher than clasp fastenings. Clasp dentures with such fastening usually cost from 50,000 rubles, and one-sided dentures can cost from 35,000 rubles. The price of clasps usually includes the cost of crowns, clasps and the prosthesis itself.
Currently, clasp prosthetics is one of the best, reliable and aesthetic types of restoration of missing teeth. Often, the only alternative to this type of treatment is the expensive and not accessible method of dental implantation. However, what type of prosthetics you prefer is up to you and your orthodontist to decide. Health to you and your teeth.
Sources used:
- I. Yu. Lebedenko Orthopedic dentistry, 2012
- “Partial removable dentures” (Zhulev E.N.)
- Mitchell, David A.; Mitchell, Laura; Brunton, Paul (2005). Oxford handbook of clinical dentistry
Manufacturing stages
This type of prosthesis is quite labor-intensive to manufacture. The process takes a long time, it includes the following laboratory steps:
- Making a plaster cast. Thanks to this, you can choose the right design taking into account individual characteristics.
- Determination of bite and jaw position in three cavities.
- Carrying out measurements of the load on the supporting teeth.
- Creating a drawing of a prosthesis on a model. This allows you to determine design features.
- Grinding teeth on a model..
- Creating a plaster prototype using a cast. .
- Frame casting, grinding and polishing. At this stage, a wax model and a special alloy are used.
- Installation of artificial teeth on a wax roller. This is done in order to obtain their fingerprint. .
- Preparation of a wax model impression, which is then poured.
Fixation
An attachment is a mechanical detachable connection. One of its two parts is fixed on the tooth, and the second is inserted into a metal frame. The locks are completely invisible and reliable. They snap into place after the denture is inserted into the oral cavity. There are no metal hooks on the front surface of the teeth, as with clasp dentures, so the locking fastenings of clasp dentures are the most aesthetic.
Locks are divided into three types - hinged, rotary and rigid. The choice of a particular option depends on the location of the dentition defects. Dentures are easy to remove for cleaning.