Neurologist (algologist)
Vasilenko
Marina Gennadievna
Experience 26 years
Head of the Pain Treatment Center, neurologist-algologist, member of the Society of Neurologists and Neurosurgeons, Russian Society for the Study of Pain, Association of Interdisciplinary Medicine, International Association for the Study of Pain (IASP)
Make an appointment
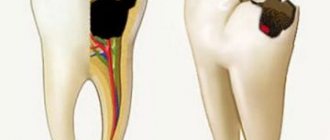
The trigeminal nerve is the largest of the 12 cranial nerves, specifically their fifth pair. It belongs to the nerves of a mixed type and includes very sensitive fibers. This name is due to the fact that the nerve is divided into three branches, providing mobility and sensitivity of the face, mucous membranes of the mouth and teeth. These are the ophthalmic, maxillary and mandibular branches.
Inflammation of the trigeminal nerve is a serious pathology that causes severe pain in the facial area. Otherwise it is called neuritis. In turn, neuralgia is pain along the trigeminal nerve. It can act as an independent sensitivity disorder, but it often accompanies inflammation, i.e. neuritis.
Symptoms and signs
Acute trigeminal neuralgia causes sudden and very severe pain along the nerve fiber. It manifests itself in attacks and is shooting and burning in nature. On average, the duration of an attack is up to 3 minutes; in approximately 7% of patients it lasts up to 3 days. Their number can reach 200 per day.
Pain from trigeminal neuralgia can be observed in different parts of the face. It all depends on which branch of the nerve was affected:
- if maxillary - in the area of the facial muscles, upper jaw and nose.
- mandibular – the pain will resemble a toothache.
- ophthalmic – in the area of the temples, forehead and above the eyebrows.
Against the background of pain, the patient develops increased anxiety and even phobias. A person strives to avoid those poses and movements that provoke unpleasant sensations in him. Other characteristic symptoms of inflammation of the trigeminal nerve:
- facial muscle spasms;
- increased salivation;
- increased or decreased sensitivity of facial skin;
- moderate increase in temperature;
- weakness and muscle pain.
Are you experiencing symptoms of trigeminal neuralgia?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Symptoms
The first attack of pain can be triggered by elementary things that no person can do without: laughter, smiling, articulation, brushing teeth, eating, frostbite on the face. Pain appears in one half of the face. At first, the painful attacks are short-lived. They end, just as they begin, abruptly. Over time, pain occurs more frequently and lasts longer. Often the pain begins to originate in the jaw and can be confused with toothache. Then the painful sensations move to the area of the cheek, ear, and forehead. There is lacrimation, paresis of the facial muscle, and the face becomes asymmetrical. After the attack, a period of remission occurs, which lasts several minutes. During remission there is no pain.
Causes and risk factors
Neuralgia of the trigeminal nerve branch is a disease with many possible causes. First of all, this is compression by vessels: displaced arteries or veins. Inflammation can also be provoked by metabolic disorders and diseases that are associated with them. These are diabetes mellitus, gout and other similar pathologies.
There are other possible causes of trigeminal neuralgia:
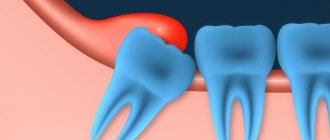
- inflammations that occur during dental treatment;
- hypothermia (general or facial area);
- mental disorders;
- purulent diseases of the jaw bones or skull;
- infection of the body with worms;
- chronic caries or sinusitis;
- infectious and viral diseases (herpes, adenoviruses, mumps, pulmonary tuberculosis, herpes zoster);
- very severe allergies;
- brain tumors;
- inflammation of the outer, middle or inner ear;
- multiple sclerosis;
- too narrow canal of the facial nerve from birth;
- injuries or operations on the temporal bone.
Possible complications
Over time, symptoms of inflammation of the trigeminal nerve can give rise to neuropathic complications and lead to the development of secondary pain syndrome in the head. In the chronic form of the disease, the auditory and facial nerves are irritated. Without treatment, trigeminal neuralgia can lead to more serious complications:
- dystrophy of masticatory muscles;
- decreased sensitivity of the affected area;
- Sykinesia (cooperative movements in which one nerve controls many muscles);
- contracture and spontaneous contraction of the facial muscles;
- conjunctivitis.
Symptoms of neuralgia
- Facial pain (prosopalgia). A characteristic sign of neuralgia. Sharp and sudden, reminiscent of an electric shock. Usually lasts from 5 to 15 seconds, is paroxysmal in nature and can occur at any time. During periods of remission, the number of attacks decreases. Most often, pain occurs in the area of the cheekbones and lower jaw (both right and left), and can be localized in almost all areas of the face.
- Impaired sensitivity. A severe form of neuralgia can lead to partial or complete loss of sensitivity of the skin.
- Nervous tic of the eyelid (nystagmus), spasms and twitching of facial muscles.
- Loss of coordination and motor skills are rarer manifestations of severe forms of the disease.
- Headaches, fever, chills and weakness are syndromes caused by viruses and infections.
When to see a doctor
If you experience symptoms of trigeminal neuralgia, you should immediately consult a doctor, as it may be a sign of another serious disease. In the treatment of neurological pathologies, accurate and timely diagnosis is extremely important. This is done by a neurologist, with whom you can make an appointment at our clinic in the center of Moscow. The specialist knows not only how to relieve trigeminal neuralgia, but also how to correctly diagnose it in order to prescribe effective treatment in the future.
Diagnosis of trigeminal neuralgia
A preliminary diagnosis can be made by a neurologist based on the patient’s complaints, studying the history of his disease and an objective examination of the face with an assessment of symmetry at rest and when trying to smile. Also, during the consultation, the doctor may conduct additional tests, asking the patient to close his eyes, purse his lips, frown, etc.
Laboratory and instrumental diagnostics of trigeminal neuralgia include the following examinations:
- general blood and urine tests;
- computed tomography (CT) and magnetic resonance imaging (MRI);
- radiography of the paranasal sinuses;
- panoramic radiography of the oral cavity;
- electroneuromyography to determine the localization of inflammation.
- Surgery
- Oncology
- Neurosurgery
- Radiology and Radiation Therapy
- Gynecology and new reproductive technologies
- Traumatology and Orthopedics
- Cardiology
- Neurology
- Laser surgery
- Urology, andrology and microsurgery
- Plastic surgery
- Mammalogy
- Lithotripsy
- Psychological support service
- ECO
- Weight loss
- Pressure chamber
- Endovascular surgery
- Pituitary adenomas
- Arnold-Chiari malformation and syringomyelia
- Parkinson's disease
- Hydrocephalus
- Hemifacial spasm
- Herniated discs
- Violent movements
- Brain tumors
- Vascular diseases of the brain
- Trigeminal neuralgia
- Glossopharyngeal neuralgia
- Essential tremor
The trigeminal nerve (V pair of cranial nerves) contains sensory, motor and autonomic fibers (Fig. 1). The nuclei of the trigeminal nerve are located in the brain stem, at the exit from which the fibers that make up the large root reach the top of the pyramid of the temporal bone, where the trigeminal ganglion (Gasserian ganglion) lies, from which 3 branches extend: the orbital (sensory) nerve leaves the skull through the superior orbital gap, innervates the upper eyelid, conjunctiva of the eye, skin of the forehead and scalp in front; the maxillary (sensitive) nerve leaves the skull through the round foramen, penetrates the pterygopalatine fossa, innervates the skin of the lower eyelid, cheeks and nose, mucous membrane of the nasal cavity, upper jaw, etc.; The mandibular nerve (the small root of the trigeminal nerve, containing motor fibers, joins it) leaves the skull through the foramen ovale, innervates the skin of the lower part of the face, the mucous membrane of the cheeks, tongue, lower jaw, masticatory muscles, etc. The trigeminal nerve takes part in many reflexes ( corneal, mandibular, etc.). Fig. 1 Anatomy of the trigeminal nerve and its branches. Trigeminal neuralgia is a disease accompanied by paroxysmal intense unilateral facial pain in the area of the chin, lips, gums, cheeks, eyes, lasting several seconds or minutes. As a rule, middle-aged and elderly people suffer. A characteristic feature is the ability to cause pain by touching a specific area of the face or mouth.
Clinic and diagnostics.
The first attack of pain seems subjectively so pronounced and unexpected that, as a rule, patients well remember all the circumstances of the initial paroxysm even after many years. Sometimes the disease begins gradually with a slight unpleasant feeling of twitching, “electrification” in a certain area of the face, or with a toothache, which forces you to seek help from a dentist. Only the characteristic paroxysmal pain that subsequently appears allows a correct clinical diagnosis to be made and appropriate examination and treatment to be carried out. Trigger zones for the development of an attack (trigger zones) with trigeminal neuralgia are localized close to the midline, covering the lips, wings of the nose, eyebrows and chin, in rare cases located in the external auditory canal. Localization of trigger zones on the gums, tongue and palate makes it impossible to eat, talk, and perform basic hygiene requirements. Some patients with a similar arrangement of the trigger zones and severe pain lose weight, become weak and fall into a depressive state, sometimes leading to suicide attempts. The attacks recur day and night for several weeks, and then often subside. After some time, the disease appears again, and after a few years the attacks become permanent. The diagnosis of trigeminal neuralgia is confirmed by relief of pain when taking carbamazepine drugs (finlepsin, tegretol). After several years of taking carbamazepine, the effectiveness of the previous dosage usually decreases and there is a need to increase the dose of medication. Some patients cannot tolerate this drug due to side effects such as drowsiness, dizziness and staggering when walking, pain in the liver, suppression of white blood cells (leukopenia). The cause of such facial pain in most cases is compression of the trigeminal nerve root by an arterial vessel at the level of the posterior cranial fossa. Less commonly, trigeminal neuralgia can be caused by brain tumors or multiple sclerosis. Trigeminal neuralgia in multiple sclerosis, tens of times lower in frequency than typical trigeminal neuralgia, occurs as a result of demyelination of trigeminal sensory structures, mainly the entrance zone of the sensory root and the descending tract of the trigeminal nerve. It is likely that the subsequent replacement of foci of demyelination by glial cells, causing an increase in the excitability of neighboring sensory fibers, also contributes to the persistence of the pain syndrome. In addition, the development of trigeminal neuralgia in patients with multiple sclerosis may be due to vascular compression of the trigeminal sensory root. Trigeminal neuralgia in brain tumors can occur with tumors of the posterior and middle cranial fossa, pituitary tumors, epidermoids in the case where tumor growth leads to direct compression of the trigeminal nerve root or changes the spatial relationship of vessels and nerves in such a way that one of the vessels leads to compression of the trigeminal nerve root (Fig. 2). Fig. 2 Trigeminal neuralgia with epidermoid tumor. Intraoperative photography. 1 – tumor. 2 – trigeminal nerve root. To exclude a brain tumor, vascular pathology, or multiple sclerosis, all patients undergo magnetic resonance imaging (MRI) of the brain. Often in such photographs you can see the “culprit” vessel compressing the trigeminal nerve root.
Treatment.
The diagnosis of neuralgia is confirmed by relief of pain when taking carbamazepine drugs (finlepsin, tegretol). After several years of taking carbamazepine, the effectiveness of the previous dosage usually decreases and there is a need to increase the dose of medication. Some patients cannot tolerate this drug due to side effects such as drowsiness, dizziness and staggering when walking, pain in the liver area. Surgical treatment is indicated for patients who cannot tolerate carbamazepine drugs or when their effectiveness decreases. Our center is a leading institution in Russia performing all types of surgical interventions for trigeminal neuralgia with more than 20 years of experience in the diagnosis and treatment of this disease. A method of treating pathology that has proven to be highly effective is percutaneous radiofrequency trigeminal rhizotomy, an operation that involves partial destruction of the trigeminal nerve root under local anesthesia. The procedure is carried out as follows: a) a thin needle is passed through the face to the base of the skull under X-ray control (Fig. 3). Fig. 3 Percutaneous high-frequency trigeminal rhizotomy in a patient with trigeminal neuralgia of the I-II branches. Intraoperative radiography (lateral projection), confirming the correct position of the curved electrode b) stimulation of the root is carried out, which is accompanied by a pain attack in the “sick” area of the face. This stage of surgery is the most unpleasant for patients. c) partial destruction of the root is carried out due to setting an increased temperature at the tip of the needle until sensitivity in the desired area of the face decreases. Such an operation may be preferable for elderly people, those who are afraid of open surgery, and those with multiple sclerosis. In most patients, after a few years (on average 5–7 years), the numbness in the face disappears, and facial pain reappears. A more physiological operation that does not lead to numbness in the area of innervation of the trigeminal nerve is the operation of vascular decompression of the facial nerve root (Microvascular decompression). This is a microsurgical operation performed under general anesthesia, in which, after performing a small trepanation behind the ear on the side of pain, the vessel is diverted from the trigeminal nerve root in the posterior cranial fossa (Fig. 4 and 5). The effectiveness of this technique is more than 90% if patients are correctly selected for surgery. Fig. 4 Intraoperative photo of a patient with trigeminal neuralgia. The arrow indicates compression of the input zone of the trigeminal nerve root by the loops of the superior cerebellar artery (V - trigeminal nerve, SMA - 2 branches of the superior cerebellar artery, CV - petrosal vein) Fig. 5 Intraoperative photo: decompression of the input zone of the trigeminal nerve root at the brain stem was performed (V - trigeminal nerve, SMA - loop of the superior cerebellar artery, M - fragment of muscle tissue) The recovery process after microvascular decompression surgery rarely takes more than a week, after which patients are discharged home and forget about their disease forever.
Treatment
Treatment of inflammation of the trigeminal nerve is carried out depending on the severity of symptoms. First, conservative therapy is prescribed. If this does not help, doctors resort to surgical methods. Their essence is to eliminate the cause of neuralgia. This may be compression of the nerve by the vessel. Surgical treatment is carried out using radiofrequency destruction, microvascular decompression or percutaneous surgery.
What drugs are most effective for the treatment of trigeminal neuralgia:
- antibiotics. Prescribed for infectious nature of the disease;
- glucocorticosteroids. Relieves severe inflammation in the body;
- non-steroidal anti-inflammatory drugs (NSAIDs). Helps suppress inflammatory processes;
- painkillers. Relieves soreness in the facial muscles;
- muscle relaxants.
To improve metabolic processes in the nervous tissue, the patient is prescribed B vitamins. How to relieve acute pain with trigeminal neuralgia:
- use anticonvulsants;
- provide physical rest, preferably bed rest;
- Apply an anti-inflammatory ointment or a warm compress to the site of pain.
Treatment of neuralgia
Treatment of neuralgia is a long and difficult process, but doctors at the CELT Pain Clinic know how to carry it out with maximum positive effect. For this purpose it is used for the treatment method.
Conservative method
Conservative treatment involves taking medications:
- antispasmodics;
- anticonvulsants
Radiofrequency rhizotomy
- Cost: 35,000 rub.
- Duration: 15-30 minutes
- Hospitalization: 2 hours in hospital
More details
It is very important to correctly calculate the dosage of medications and take them regularly, since this is the only way to achieve the desired effect. It is equally important to regularly attend physiotherapeutic procedures:
- Bernard currents;
- acupuncture;
- paraffin applications.
If this treatment method does not bring the desired effect, the attending physician may decide on surgical treatment.
Home remedies
Before treating trigeminal neuralgia at home, you should consult a doctor, since many remedies can only worsen the situation. If the specialist allows it, it is also possible to use various home recipes.
According to recommendations for trigeminal neuralgia, it is worth consuming orally or lubricating the affected side with birch sap. You need to drink 4-5 glasses per day. Heated buckwheat folded in cotton cloth will help relieve pain. The compress is made 2 times a day, keeping it at the site of inflammation until it cools down. At home, it is useful to massage the sore area: rub, stroke and lightly knead the area of inflammation.
Pain relief for occipital neuralgia
Damage to the nerve fibers of the cervical plexus - this disease occurs most often due to a complex of dystrophic disorders in the articular cartilage (cervical osteochondrosis). Shooting acute pain, manifested in paroxysms, goes from the neck to the back of the head. Thyme tincture helps to remove it. To do this, pour 50 g of thyme into 100 g of vodka and leave for 5 days. Take 15 drops of the prepared solution orally, after diluting it in 100 g of water, three times a day.
For external use, oil made from fir cones and young shoots is used. The oil is rubbed into the local area of pain using a gauze pad 6–8 times a day. For the same purposes, an infusion of marshmallow root is suitable, which is prepared as follows: 10 g of raw material is crushed and poured into 1 tbsp. warm water, then leave for 6–8 hours. Moisten a soft cloth with the decoction and apply it to the place where the pain is felt the most. A warming bandage is applied on top.
Myths and dangerous misconceptions in treatment
Due to the fact that neuralgia does not affect the general condition of the body, many patients postpone visiting a doctor and treating the trigeminal nerve. In fact, this is the wrong approach, since the disease can lead to paralysis and muscle paresis. In addition, it has a significant impact on psychological and social aspects of life.
No less important is the fact that painkillers for trigeminal neuralgia provide only a temporary effect. Over time, anticonvulsant medications may also stop working as they become addictive. Therefore, you should not abuse medications. They only relieve the symptoms of neuralgia, and its cause can only be identified by a qualified specialist.
Prevention
There is no specific prevention against neuralgia. Doctors only recommend eliminating as much as possible exposure to the body of those risk factors that can lead to nerve inflammation. To avoid this, it is necessary to prevent hypothermia of the face, especially in the summer when using fans and air conditioners. It is important to harden yourself and worry less in order to reduce the impact of stress. It is also imperative to treat underlying diseases that are risk factors for neuralgia.