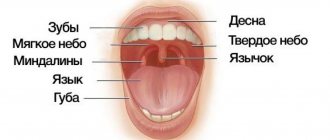
Teeth are bone formations whose main purpose is the primary mechanical processing of food. In most cases, an adult has 32 teeth. In addition to performing the chewing function, they influence the formation of human speech. The loss of baby teeth and the appearance of permanent teeth occurs after the baby’s fifth birthday - there are four types: incisors and canines, molars and premolars.
On one side of the upper jaw there are the following teeth: 1 canine and 2 incisors, as well as 2 premolars and 3 molars. The opposite side is similar to the upper one, and the arrangement of the lower jaw teeth is identical to the upper row of teeth. The condition of teeth indicates a person’s health, and if it is unsatisfactory, this may indicate some kind of disorder in the body.
READ ALSO: location of teeth in adults and their numbers
Human dental formula
Many people have heard that dentists call teeth by different numbers. Thus, each unit is assigned a specific number, which guarantees maximum accuracy in records of dental conditions or treatment procedures. The count is made starting from the middle of the dentition to the right and left sides. The anterior units - incisors - are No. 1 and 2, 3 - canines, 4-5 - premolars, 6, 7 and 8 - molars, the last of which is the wisdom tooth.
To determine exactly where the tooth is located, the jaw is figuratively divided into segments. The beginning of the numbering is the right side of the upper jaw of the teeth. Units are written as two-digit numbers, where the first determines the serial number, and the other determines the so-called segment. The upper right half of the teeth is designated by numbers 11-18, the left - 21-28, and the lower left segment - 31-38 and 41-48. Regarding primary teeth, the count is made starting from the front units on the left in a clockwise direction. They are assigned the numbers 50, 60, 70 and 80.
READ ALSO: structure of the human upper jaw and functions of its processes
There are several types of numbering that dentists use:
- With the square-numeric Zsigmondy-Palmer method, Arabic numerals are used for radical units, and Roman numerals are used for dairy units. Often used by orthodontists and surgeons.
- Haderup's method is based on the symbols "-" and "+", where the first denotes the lower and the other the opposite arc. Units are written in Arabic numerals, and in the case of dairy units, 0 is added.
- The Viola system uses Arabic numerals 1-8 for units and two-digit numbers for segments. This type is very convenient, which is why it is widely used by dentists around the world.
- The last system is universal. Each group of units is assigned a letter, number and segment number.
The structure of the upper and lower teeth
The elements of a human tooth are: crown, neck and root. The crown is visible to the naked eye - it is located above the gum. The connecting link between the tooth root and the alveolus is connective tissue. The neck of the tooth is located between the crown and the root.
READ IN DETAIL: dental formula for adults and children
From a histological point of view, the constituent basis of the human tooth is dentin, hidden under the enamel. Near the root, where there is no enamel, there are fibers that seem to hold the periodontium together. In the center of the unit there is a pulp, which is penetrated by blood vessels and nerve endings. With inflammation or caries, it makes itself felt with severe pain.
Incisor and canine crown
Both the lower incisor and its antagonist have similar components: the root and the crown. Slightly above the alveolar layer is the enamel crown of the tooth. The root of the tooth is located in the alveolar cavity under the gum (we recommend reading: how many roots does a person have in his teeth?). The large dimensions of the upper incisor are about 21-23 mm, while the length of the crown is 9-95 mm, and the width of the teeth is 4-6 mm, so the pressure on them is distributed evenly. The enamel is protected from physical damage and mechanical stress. The lateral (or lateral) incisor, in comparison with the medial one, has a huge root and a wide crown.
Content
- Features of fangs
- What to choose?
- Which implantation to choose?
- How is implantation performed?
- Perform triple implantation
A canine is a single-rooted tooth used for grasping, holding and tearing food. Humans have a pair of fangs on the upper and lower jaws. They are called "triples" because they are considered third after the two incisors. These teeth are tall and cone-shaped.
PROMOTION
Osstem dental implantation turnkey
18,000 rub.
What are baby teeth?
The formation of baby teeth begins when the baby is in the womb, namely at the 7th week of pregnancy. Teething begins when the baby reaches 6-24 months. The change from temporary units to permanent ones is carried out at the age of 5-13 years. The complete formation of a permanent dentition is completed by the age of 14. A deviation of no more than one year is acceptable. If the period of teeth replacement is exceeded, this indicates anomalies in the dental arch or jaw formation.
Structural features
Milk teeth are similar to permanent teeth, but are much smaller in size and have short, rounded roots. The thickness of dentin and enamel is also less. Due to low mineralization, teeth are susceptible to the rapid development of caries. It is worth noting that temporary units are characterized by a considerable volume of pulp and wide root canals, which facilitates the penetration of harmful microorganisms into the pulp.
The number of roots in baby and permanent human teeth is identical. When the time comes to replace temporary teeth with permanent ones, the roots of baby teeth dissolve, thereby making room for new ones. Their change is almost painless, since they are not strongly attached to the alveoli.
READ ALSO: The number of teeth of an adult healthy person is normal
Differences from permanent
Despite the similarities between milk and permanent units, there are a number of differences. First of all, this is the number of units - in contrast to permanent ones (32), temporary ones are only 20. In addition, children do not have premolars, and there is only one molar. There are also other differences:
- smaller crown
- thin enamel, white-blue color,
- dentin composition with a lower degree of mineralization,
- roots are branched and massive,
- deep fissures,
- the roots are bent closer to the lip, they are not so strong and shorter.
Aesthetic objectives: canines in the lateral incisor position
Very often, dentists do not think about the long-term consequences of their treatment. An incomplete treatment plan or poor treatment choices (often dictated by the patient) usually lead to more serious problems years later. If only we could know what will happen in the future, it would make the task much easier.
However, dentistry can be a predictable subject if approached with proper function and aesthetics in mind. Each dental student receives a phantom - a model that shows the ideal condition and position of the teeth. All dentists are taught the principles of balanced occlusion and the importance of reducing destructive forces.
This article will demonstrate what happens when the factors of time and aging are not taken into account when choosing a treatment method. Very often, what patients themselves do not notice or consider unimportant, about which they do not complain, can turn into a real problem only several years later. If we, dentists, approach the patient from the standpoint of individuality and at the same time as a component of one population, if we carry out careful planning and elaboration of parameters, striving for that same phantom model, then we come to a predictable and long-term quality result. The clinical case discussed here concerns a woman with congenital absence of lateral incisors. When she was a teenager, the maxillary canines were orthodontically moved into position as lateral incisors. In her younger years, her appearance was quite harmonious and attractive, but over time the picture began to change.
Absence of lateral incisors
It is reported that approximately 2% of the population are congenitally missing one or two lateral incisors. Paired absences are more common, and if only one is present, it is usually a microdent. Performing OPTG at an early age makes it possible to find out which of the permanent teeth have not formed.
It is very important to learn about the congenital absence of a tooth at an early age, so that the entire sequence of therapy can be correctly coordinated to restore aesthetics and function. Treatment of congenital absence of lateral incisors is an orthodontically and therapeutically complex task, which is based on the tooth-dental arch size relationship. Numerous studies have been published comparing the method of mesial repositioning of canines and distalization of canines followed by prosthetic restoration of missing incisors.
From a modern point of view, the most logical way is, of course, to open up space and replace missing teeth with prosthetics. The phantom from student life, at least, definitely had his own lateral incisors.
Moving the canine to the lateral incisor position may have several aesthetic and functional disadvantages:
- The canine, a fairly wide tooth, begins to replace the naturally narrow incisor. The color of the canines is usually somewhat darker than that of the lateral incisors, so they stand out from the general plan if they are not in the corners of the smile.
- The level of the gingiva of the canines is approximately similar to that of the central incisors, so moving the canine to the place of the lateral incisor causes visual disharmony.
- Insufficiency appears in the processes of occlusion and articulation, since after movement the canine guidance of the lower and upper canines is not carried out together.
- In the absence of canine protection, the risk of abrasion of the remaining teeth increases, usually consisting of small cracks and microfractures. Over time, periodontal problems and increased sensitivity may appear.
- Long-term retention with an orthodontic retainer will be required to retain the canine in the lateral incisor position.
- The patient may begin to experience TMJ discomfort, muscle tension, grinding, and headaches. This may occur due to effects on muscles that are not anatomically intended.
- The tissues of the vestibule of the oral cavity and the bony prominence in the area of the canine root do not look natural in the area of the lateral incisor. Without the presence of a tubercle in the corners of the mouth, the tissues do not have sufficient support, which leads to recession of the cheeks and narrowing of the buccal corridors. Over time, fewer and fewer teeth become noticeable when smiling.
Orthodontic vision
Traditionally, orthodontists have not encountered people in need of restorations, as they have primarily worked with younger patients. Young people rarely need major restorations. However, in the 21st century, orthodontists often began to take on patients with the need for restoration or due to periodontal disease in the latter. The absence of a lateral incisor is an aesthetic indication, so the orthodontist should treat such a case in this aspect.
The goals of orthodontic treatment often vary depending on the final goal and the need for restoration:
- Positioning of teeth can occur in order to improve the performance of any restoration, for example, to replace a lateral incisor or another tooth.
- There are some advantages to performing permanent or temporary restorations before, during or after orthodontic intervention. This restoration allows you to create the desired shape and at the same time gives an idea of the required space and dimensions. Tooth wear, fractures, underdevelopment in the form of barrel-shaped incisors, etc. are the main indications for restoration before orthodontic treatment.
- Orthodontists sometimes need to reposition a tooth to improve oral hygiene
- Orthodontic treatment may be performed due to periodontal problems, such as insufficient gingival margins, absent gingival papilla, or bone loss.
Today, the goals of orthodontic treatment have diversified significantly, as the aesthetic and functional vision of problems has expanded. Properly planned orthodontic treatment can achieve stable and functional occlusion, improve the health of periodontal tissues and improve dental and facial aesthetics. Orthodontists simply need to study facial aesthetics. Modern specialized literature, research and training always have a positive effect on a specialist and, accordingly, his work results. However, in the past, very little attention was paid to facial aesthetics and periodontal tissue health. A successful orthodontic treatment can be considered an intervention that results not only in the ideal articulation of the models (as well as the achievement of ideal cephalometric relationships and sizes), but also in the restoration of facial aesthetics and harmony in a given position of the teeth.
A smile analysis should include the following: the vertical position of the teeth at rest and when smiling; the transversal (horizontal) dimensions of the smile; the characteristics of the smile arc; and the vertical relationship of the gingival margins to each other. Taking into account all the data, it becomes desirable to move the canines to their natural position and replace the lateral incisors through prosthetics.
Interdisciplinary treatment planning
Innovations in aesthetic dentistry have led to developments in all dental specialties. In today's standard of dental rehabilitation, specialists proceed, first of all, from the individual characteristics of the patient's face and his needs. Each treatment plan begins with an aesthetic assessment. During the analysis, the patient's lips, skin, and cheeks are examined. We must always refer to the position of the teeth in the upper jaw and the level of the gums in relation to the face, and then determine what corrections need to be made for a given appearance. We cannot achieve correct occlusion until our final vision of aesthetics is determined. Aesthetics dictates where the teeth should be located, what the vertical position, guidance and relationship should be.
The main person in the team is the restorative dentist, and the success of teamwork is achieved through detailed discussions of each problem. The main specialist must achieve real therapeutic goals (take into account the economic component, expectations), create an aesthetic vision of the final result, determine the sequence of treatment and restore poorly formed teeth to ideal proportions. The restorative dentist acts here as a link among all specialists, uniting and controlling the manipulations carried out and the pursuit of the final goal.
Clinical case
Diagnosis and treatment plan
A 40-year-old woman came to the clinic (in 2003) in need of cosmetic correction of treatment performed in adolescence.
The patient had a congenital absence of lateral incisors, so she underwent orthodontic treatment at the age of 14 years to solve this problem. Relying on the orthodontist and unaware of other treatment options, the parents chose (or allowed) to move the girl's canines to the lateral incisor position. After the treatment, the smile did not look attractive enough, but the patient was able to get used to it. But as she reached middle age, the woman began to notice that her interlocutors were increasingly staring at her teeth. This made her insecure. The canine was darker, had a rounded contour and a gum level that was in disharmony with the rest of the teeth. The buccal corridors were narrowed to close the empty space, creating the appearance that the cheeks were somewhat sunken (Photos 1 and 2). The patient remained deeply dissatisfied with her appearance.
Photo 1: In 2003, a 40-year-old patient presented with an aesthetic problem.
Photo 2: The canines were moved to the position of the lateral incisors, which stood out from the overall appearance.
With the advent of the 21st century, there have been significant changes in dental technology and materials. Aesthetic manipulation has become common and routine. In this situation, should we have moved the canines to their correct position and replaced the lateral incisors? The patient was open to any options.
After weighing all our options, we decided not to move the canines back and place titanium implants. Although this would be the most common solution to the problem, this path did not seem entirely justified to us. Such treatment would take approximately 18 months, and there was also the possibility of resorption and the need for bone grafting. Since the patient clearly wanted to change the shape and color of her front teeth, an easier and more predictable alternative was in development.
After analyzing radiographs, photographs and working models, we decided that after flattening and narrowing the canine, we could use light orthodontic extrusion of the teeth, which would realign the ridge bone and create a new harmonious appearance at the soft tissue level. By leaving space distal to the canine, we can create porcelain veneers to correct the shape of the canines to resemble the lateral incisors and the first premolars to resemble the canines. Placing veneers on the side teeth will also be possible if the patient so desires. According to the plan, the treatment was supposed to take approximately 6 months. It is important to evaluate all the benefits and risks of any of the treatment options, and the chosen option already needs final approval by the patient himself.
Since the patient expressed a desire to install veneers on the teeth of the anterior zone, all we had to do was correct the position of the lateral incisors and canines.
Clinical protocol
The labial surface of the canines was flattened and the mesial and distal contours were tapered using a flame-shaped diamond bur (Dental Savings Club) followed by finishing with strips (Integra Miltex). Ormco Saphire (Ormco) braces are fixed on the upper jaw up to the first molar (Photo 3). Using Ni-Ti wires of increasing diameter from 0.13 to 0.16 with an extrusion force of 15 g, it was decided to carry out labilization of the central incisors and extrusion of the canines to correct the gingival level (Photo 4). The use of orthodontic extrusion to modify soft and hard tissues was first described in the literature by Heithersay and Ingber. Low-intensity forces (up to 30 g) stimulate marginal positioning of the bone crest, behind which movement of the gums occurs. Restructuring of the alveoli occurs along with the movement of the root.
Photo 3: Preparation for orthodontic treatment: the labial surface of the canines was slightly flattened, and the contours on the proximal sides were narrowed.
Photo 4: Ni-Ti arch with a force of 15 g is used to labilize the central incisors and extrusion of the gingival level of the canines.
Extrusion of the canines by 1 mm was carried out over 3 months, followed by stabilization for 3 months with a Ni-Ti arch 18x25. The total time spent on treatment coincided with the plan and amounted to 6 months. The gingival level of the canines is corrected and lowered, the canines are ready for restoration according to the proportions of the lateral incisors. For the formation of “fangs” from premolars, space is left distal to the true canines (Photo 5a-6). The braces are removed, leaving the teeth in an ideal position for further restoration with porcelain veneers (Photo 7).
Photos 5a and 5b. Reduced gingival level at the lateral incisor.
Photo 6: Space is left at the distal surface of the canine for restoration of the premolar in the shape of the canine.
Photo 7: After removing the braces, the teeth are left in an ideal position for further restoration.
A vinyl polysiloxane (VPS) impression was made, followed by a diagnostic wax-up of the anterior 6 teeth (Figure 8). At this stage, it was decided to evaluate the esthetics of the anterior sextant before widening the buccal corridor.
Photo 8: Diagnostic wax-up creating the ideal appearance of the 6 front teeth.
Conservative preparation (0.3 mm) was carried out (Photo 9) and the final VPS impression was taken (Honigum DMG America) using conventional and lightweight techniques. Bite registration was carried out by Luxabite (DMG America). Using the classic VITA scale, shade A1 was determined. Temporary structures made of bis-acrylic material (DMG America), made on the basis of a diagnostic wax-up matrix, are fixed to the prepared teeth. Fixation was carried out using Temp Bond Clear (Kerr). Next, the appearance of the structures was corrected with soft diamond and Flexi discs (Cosmedent) (Photo 10).
Photo 9: The teeth were prepared by 0.3 mm to install ceramic veneers.
Photo 10: Luxatemp temporary structures (DMG America), creating a natural smile appearance.
Models are cast from plaster (Photos 11a and 11b) and then porcelain veneers are made (Photos 12a and 12b).
Photos 11a and 11b. The Geller technique allows you to emphasize the contour and level of the gums.
Photos 12a and 12b. Veneers made from Creation Porcelain (Jensen Dental).
The veneers were fixed with colorless cement (Variolink Veneer Ivoclar Vivadent) in 2004. The patient was satisfied. Ultimately, she adjusted her smile to the desired result. The size and shape of the front teeth are made according to golden proportions, so it is almost impossible to determine the congenital absence of incisors. Premolars are shaped like canines. At this stage, the slightly reduced buccal corridor did not bother the patient at all.
After some time
Ten years later, in 2013, the patient returned to the clinic. Now the lateral teeth caused aesthetic dissatisfaction (Photo 15). The upper second premolars and molars on both sides were prepared (Photos 16a and 16b), then a suitable shade was selected (Photo 17). The restorations were made from Creation Porcelain (Photo 18). The structures were fixed using transparent cement for veneers (Variolink Veneer). The resulting result looked uniform, as if created at the same time (Photos 19 and 20). The patient was satisfied.
Photo 13: Completed treatment in 2004.
Figure 14: Despite the narrowing in the lateral areas, the patient was satisfied with the aesthetics of the anterior segment.
Photo 15: By 2013, the patient wanted fuller buccal corridors.
Photos 16a and 16b: Preparation of second premolars and first molars.
Photo 17: Shade selection according to the VITA scale.
Photo 18: Making ceramic restorations (Creation Porcelain).
Photos 19 and 20: Completed treatment in 2013.
Final comment
People often change their minds, so it is difficult to predict what a patient who was treated as a teenager will want. A careful treatment plan helps overcome many of the negative factors associated with subsequent gradual aging. A careful discussion of all the details allows for high-quality rehabilitation, as well as building a trusting relationship with the patient.
Author: Elliot Mechanic , DDS, BSc