The term “alveoli” in dentistry refers to anatomical pits located in the upper and lower jaws and necessary for fixing teeth. Another name for alveoli is dental sockets. The dental socket is filled with connective tissue (collagen fibers with a low degree of elasticity) that surrounds the tooth root and connects the root cement to the alveolar bone plate. The holes are separated from each other by interalveolar plates, and in total there can be from 28 to 32 alveoli in a person’s mouth (according to the number of teeth). The most serious pathologies of dental alveoli are alveolitis, as well as periodontal and periodontal diseases, which can cause a decrease in interalveolar height, loosening and tooth loss.
Location and structure
Dental alveoli (sometimes also called alveolar sockets or cells) are depressions located in the alveolar bone of the upper and lower jaw. Alveolar bone is represented by two components:
- alveolar process (anatomical part that forms the so-called “dental bed” to which all the teeth of the upper jaw are attached);
- alveolar part (anatomical bone surface intended for attaching teeth to the lower jaw).
The alveolar processes are filled with bone spongy substance, osteons (structural units) of which form the walls of the alveolar socket. Inside, the dental cells are separated by bone partitions, that is, in one hole there can be from one to three or four recesses in which the dental roots are located, surrounded by periodontal tissues. In rare cases, the number of cavities can reach five if a person is diagnosed with the eruption of abnormally modified “eights” (“wisdom teeth”) with a complex root system.
The structure of the alveolar cells is porous (due to a large amount of loose connective tissue). Nutrition of the alveolar bone is carried out by diffusion through blood vessels located in periodontal and periodontal fibers, as well as cancellous bone substance. The structure of the alveoli also contains nerve plexuses and lymphatic vessels.
What complications can the disease lead to?
Under no circumstances should such a problem be ignored. The lack of timely therapy leads to the replacement of pulmonary structures with connective tissue. The lungs gradually lose their properties, the body does not receive enough oxygen. One of the dangerous complications is hypoxia of all organ systems. Serious metabolic disorders are also possible.
Gradually, the fibrotic process leads to the development of respiratory failure. The list of dangerous complications also includes pulmonary edema, which is the result of liquid blood components entering the cavity of the respiratory organs. Edema can develop at lightning speed - often this condition ends in the death of the patient. In other cases, the pathology develops gradually - the symptoms progress slowly, the patient’s condition worsens within 24 hours, which makes it possible to call a doctor in time.
Embryogenesis
The formation of dental alveoli begins during the embryonic development of the fetus, when the formation of dental buds occurs. The rudiments of primary teeth are formed at approximately 8-10 weeks of gestation, and the formation of molars begins only at the end of the fourth month of intrauterine growth. Despite the fact that the rudiments of the teeth themselves appear only at the beginning of the third month of gestation, the elements from which they are formed are laid much earlier (up to 6-7 weeks), so in the first trimester it is important that the woman receives a sufficient amount of essential minerals: calcium, phosphorus, magnesium, iron.
Table. Embryogenesis and stages of formation of teeth and dental alveoli.
| Embryonic age of the fetus | What happens at this stage? |
| 6-7 weeks | From the epithelial cells covering the surface of the jaw, a plate-shaped growth is formed, which over time acquires an arched shape (a dental plate is formed). |
| 7-8 weeks | The plate formed in the oral fossa gradually connects with the mesodermal parenchyma of the jaw (along the free edge) and forms the enamel pulp. |
| 12-20 weeks | The enamel organ separates and the dental crown is formed from the mesodermal parenchymal components and the neural groove. |
| 16-20 weeks | The formation of the rudiments of a molar (permanent) tooth occurs, which is initially located in the same bone alveolus with milk teeth. |
Note! The permanent and primary teeth, which initially reside in a common alveolar socket, will later be separated by a hard septum. The destruction of the dental root of non-permanent (baby) teeth occurs at approximately the age of 6-12 years: the milk tooth falls out of the socket, and the entire dental cell is occupied entirely by the molar (permanent) tooth.
Mechanism of external respiration
The cells of the body are provided with oxygen and freed from carbon dioxide thanks to the blood passing through the capillary network of the alveoli. Oxygen and carbon dioxide, released from carbonate acid and its salts by the enzyme carbonic anhydrase, continuously move in opposite directions through the aerohematic barrier. It is found in red blood cells. The scale of diffusion can be judged based on the following figures: about 300 million alveoli forming lung tissue make up approximately 140 m2 of gas exchange surface and provide the process of external respiration. The above facts explain what the alveolus is and what role it plays in the metabolism of our body. In fact, it is the main element that ensures the breathing process.
Functions: what are alveolar sockets for?
The main function of the alveolar cells is to fix the tooth root and hold the tooth in an anatomically correct position. If there is an age-related decrease in the interalveolar height, trauma to the tooth socket or its inflammation, a violation of the fixation ability of the alveoli and gradual loosening of the teeth with subsequent loss are possible. Diseases of the soft tissues of the oral cavity (periodontitis, parodontitis) can also cause unreliable fixation of the tooth root, destruction and loss of the tooth from the bone alveolus.
Holding the tooth and fixing it to the jaw is not the only functional purpose of the dental socket. Alveoli are also necessary to perform the following functions:
- formation of correct diction and implementation of speech function (if even one tooth is missing in the mouth, the quality of speech can significantly decrease);
- giving the dentition a stable position;
- reducing the load on the tooth;
- preventing premature tooth decay.
It is especially important to monitor the condition of the tooth socket after tooth root extraction until it is completely healed, since various complications during this period can negatively affect the condition and health of neighboring alveoli and the teeth located in them.
What are the features of the upper alveoli of the teeth?
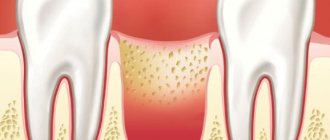
Photo: alveolitis
Regardless of which jaw the alveoli are located on, there are no significant differences in their structure. The only peculiarity of the upper alveoli of the teeth is that their structure affects diction and intelligibility of speech , which is due to the close location of the alveolar process and the palate.
The alveoli are susceptible to a number of dental diseases, the most dangerous of which is alveolitis. The disease can cause relaxation of the alveolar tissue, which can cause the tooth to shift, become loose, or even fall out. If you suspect that your teeth have begun to shift, you should immediately contact the dentist.
How many tooth sockets are there in the mouth?
The number of alveoli in humans ranges from 28 to 32 and corresponds to the number of teeth. The size, shape, and height of the alveolar fossae are individual for each person and are multifactorial indicators, that is, they depend on a combination of several factors: age, degree and quality of hygienic oral care, the presence of dental and endocrinological diseases, history of surgical treatment of teeth and gums .
Unlike teeth, the number of which can decrease with age (tooth loss or surgical extraction), the number of dental sockets is a constant value. Alveoli, which lack teeth, overgrow over time and lose their functional significance, but still remain an anatomical unit of the jaw system.
Diagnostic measures
Diagnosing alveolitis of the lungs is not so simple. To begin with, the doctor conducts a general examination. If there is wheezing and noise in the lungs, additional procedures are prescribed. The patient donates blood for analysis - during the study, antinuclear and rheumatoid factors are detected in the samples. The disease is characterized by an increase in erythrocyte sedimentation rate.
To make a diagnosis, some instrumental studies are also necessary:
- First of all, a chest x-ray is performed, since this simple and affordable procedure makes it possible to notice changes in the structure of the lungs;
- spirometry is a study that allows you to study the characteristics of the patient’s respiratory process;
- additionally, electrocardiography is performed;
- bronchoscopy is a procedure that allows you to carefully examine the structure of the bronchi from the inside;
- the most informative is high-resolution computed tomography - the study makes it possible to determine the number and location of foci of inflammation, to see changes in the size and shape of the alveoli;
- in some cases, patients are shown a biopsy, which helps determine the presence of a malignant process and other abnormalities in the lung tissue.
Defects and diseases of the alveolar sockets
Alveoli in the mouth, like other anatomical formations in the human body, can become inflamed, injured and subject to various deformations. Congenital anomalies and defects in the development of dental sockets are quite rare (less than 5.1% of cases): in the vast majority of alveolar pathologies are acquired in nature and are the result of various injuries and dental diseases.
Injuries and fractures
Traumatic damage to the tooth socket is a common complication of jaw fractures. Such pathologies can lead to irreversible deformations not only of the dental alveoli, but also of the entire dentition, so it is important to follow preventive measures if there is an increased risk of such injuries. This applies to boxers, figure skaters, speed skaters, and people suffering from pathologies of the musculoskeletal system, in particular osteoporosis.
With osteoporosis, there is a progressive decrease in bone mass, which leads to the fact that the jaw bones become fragile and susceptible to various mechanical injuries and damage. Most often, osteoporosis affects the lower jaw and is a consequence of chronic calcium deficiency. The main risk group consists of people suffering from diseases of the gastrointestinal tract (the absorption of essential vitamins and minerals is impaired), who do not follow the principles of a healthy and balanced diet and who have a history of endocrinological pathologies.
Alveolar socket cyst
Such cysts are also called odontogenic or jaw cysts. Radicular cysts, which make up more than 90% of all jaw cysts, can be located on any part of the alveolar process, and the clinical picture depends on the size of the formation and the nature of its contents. If the cyst is filled with inflammatory or serous exudate and is small in size, it can only be diagnosed after an X-ray examination of the tooth and its root.
Purulent cysts have a more pronounced clinical picture, and its symptoms are quite well defined and visualized during the initial examination. It can be:
- high body temperature exceeding febrile levels;
- unpleasant, pungent smell of rotting;
- sharp aching pain;
- bulging and deformation of the alveolar process.
Cysts of the upper jaw, if large in size, can have the clinical picture of sinusitis, as they grow predominantly towards the nasal passages and turbinate.
Dry alveolar cell syndrome
Dry socket is a pathology that develops after extraction of molars. The structure of the dental alveoli is represented by a large number of nerve bundles and capillaries, so after this operation the hole is immediately filled with blood, which, under the action of enzymes, thickens, coagulates and forms a blood clot (clot). Such a bundle has important functional significance: it protects the nerve plexuses and exposed bone areas from infection and mechanical injury, and also promotes faster healing of the alveoli and its tightening.
Damage or removal (either accidental or intentional) of a blood clot is called dry socket syndrome. It is this pathology that in 80% of cases provokes the development of post-extraction alveolitis - inflammatory changes in the soft and hard tissues of the alveolar socket, often requiring antibacterial and antimicrobial therapy and even surgical treatment.
Reasons that can lead to displacement or partial destruction of a blood clot include:
- non-compliance with a gentle regime for hygienic care of the oral cavity (active rinsing, smoking, drinking drinks through a straw, etc.);
- constant mechanical pressure on the clot (according to statistics, almost 91% of patients involuntarily touch the formed clot with their tongue, which can provoke its displacement);
- exposure to tobacco smoke.
In women, one of the causes of dry alveolar syndrome may be taking COCs.
Note! To prevent clot displacement, it is necessary to maintain a gentle hygienic and dietary regime, carefully monitor oral hygiene, avoid increased physical activity and stop smoking and drinking alcohol for at least 72 hours after surgery.
What does the treatment plan look like?
What should patients who are diagnosed with pulmonary alveolitis do? Treatment is tailored individually. Here, much depends on the form and stage of development of the disease. In any case, therapy should be aimed not only at eliminating the cause of inflammation, but also at inhibiting the fibrotic process.
- In case of allergic and toxic alveolitis, it is extremely important to protect the patient from contact with hazardous substances. Cytostatics and glucocorticoids are also used (sometimes they are administered directly into the respiratory system by inhalation).
- Patients are prescribed medications that dilute the mucus secreted by the epithelium and facilitate its passage.
- Prednisolone in small doses helps to cope with the inflammatory process.
- Autoimmune pulmonary alveolitis requires the use of immunosuppressants.
- Sometimes an oxygen concentrator is used - this helps to avoid hypoxia.
- In some cases, the doctor prescribes antibacterial medications, in particular penicillin.
Patients are also recommended special breathing exercises, which help preserve lung volume and cope with the fibrotic process.
Post-extraction alveolitis
The main cause of inflammation of the alveolar cell tissue is the displacement of the blood clot, which should protect the periosteum and nerve plexus from injury and infection. The prevalence of alveolitis is about 40% of all types of post-extraction complications (complications that arise after the removal of a tooth and its root).
Causes
Almost 90% of all alveolitis have an infectious etiology, so after tooth extraction, doctors often prescribe antimicrobial and antiprotozoal agents, as well as antibiotics, to the patient. Failure to comply with these recommendations and prescriptions, as well as insufficient or improper hygiene, can cause infectious and inflammatory changes in the injured socket.
Dentists also name a number of factors that increase the risk of post-extraction complications. These include:
- smoking (if a person cannot give up his habit for several days, it is necessary to at least carefully rinse his mouth with warm water after each cigarette smoked);
- consumption of spicy, fatty, smoked, pickled foods and alcoholic products;
- using a toothbrush with stiff bristles until the alveoli are tightened;
- incomplete removal of bone fragments, fragments of cysts, granulomas and other pathological tissues during surgery;
- failure to comply with aseptic measures in the dental office and operating room (in case of complex removal);
- active rinsing of the mouth on the first day after extraction.
Chronic diseases leading to persistent weakening of the immune system, as well as the complex nature of the removal (for example, the complex removal of the eighth molar) can contribute to the development of pathogenic flora and infection of the socket.
Clinical features
One of the main and most clinically significant signs of post-extraction alveolitis is severe toothache in the place where the extracted tooth was located. The intensity of pain during alveolitis is usually high, difficult to relieve with analgesics. In some cases, the patient cannot calmly eat, sleep and perform household and work duties, so one of the main tasks of treating alveolitis is to relieve the inflammatory process and reduce pain.
An inflammatory process after dental extraction can also be suspected based on other symptoms that appear during the first three days after surgery. These signs include:
- a strong smell of decay that does not go away after brushing your teeth;
- systemic hyperthermia (up to 38°-39° C);
- grayish coating on the surface of the alveoli;
- discharge of purulent or serous exudate from the injured socket;
- severe intoxication syndrome (headache, nausea, severe weakness, lethargy);
- inflammation, swelling and hyperemia of the soft tissues around the affected hole.
In some cases, the patient may have enlarged lymph nodes in the neck and under the lower jaw.
Treatment
Post-extraction alveolitis almost always has an acute course and can be easily treated if you consult a dentist in a timely manner (it is better to contact the specialist who performed the extraction). First, the doctor will conduct a visual examination, after which he will perform curettage of the alveolar socket and clean it of remnants of a blood clot, granulations, food and infiltrate. If necessary, drainage is carried out followed by treatment with antiseptics. After all the manipulations, a tampon soaked in an antibacterial solution is placed in the hole.
Treatment at home after emergency dental procedures is usually carried out according to the following scheme:
- antibacterial (amoxicillin 500 mg 3 times a day) or antimicrobial (metronidazole 250-500 mg 2-3 times a day) therapy;
- NSAIDs to reduce inflammation, eliminate intoxication and fever syndrome and pain;
- local treatment (rinsing) with antiseptics, for example, hydrogen peroxide 3% or chlorhexidine.
Acute pain after starting therapy usually disappears by the end of the third day, but moderate and mild pain can persist for up to 15-20 days. If necessary, the patient can receive a certificate of temporary incapacity for work, the duration of which is usually 3-5 days.
Important! The main prevention of alveolitis is to maintain the integrity and location of the blood clot, as well as providing antiseptic treatment and the necessary hygienic care. A gentle regimen should be followed for 3 days after surgery.
Video - Pain in the socket
The alveoli in the mouth, which are commonly called dental sockets, are an important anatomical element of the jaw, necessary for speech (conversation) function and the ability to chew food normally without shifting the dentition. Pathologies of the dental alveoli occur mainly after the removal of permanent teeth, but in rare cases they can occur even before the birth of a person against the background of impaired embryogenesis. Prevention of alveolitis (the main disease of the tooth socket) consists of following medical recommendations regarding the nutritional and hygienic regime, as well as timely antiseptic treatment with disinfectant solutions and antibacterial ointments.
Idiopathic form of the disease
Idiopathic pulmonary alveolitis is less common than other types of the disease, and most often men face this problem. The causes of the development of the disease are not always known - many experts believe that the inflammatory process in this case is of autoimmune origin. Due to malfunctions of the immune system, antibodies to its own cells begin to be produced.
The main symptoms of the disease are cough and shortness of breath. The intensity of the symptoms constantly increases, so patients often consult a doctor after the onset of the fibrotic process. This form of alveolitis is considered the most dangerous, since in the vast majority of cases it ends in pneumosclerosis and respiratory failure.
Prevention
In order to prevent the development of alveolitis, it is recommended to promptly and adequately treat infectious diseases, limit contact with potentially dangerous allergens, eliminate household and professional factors that may cause the development of the pathological process, observe occupational hygiene rules, and also give up bad habits.
Persons at risk for alveolitis should undergo regular preventive medical examinations.
Video from YouTube on the topic of the article:
Forecast
With timely and adequate treatment of acute exogenous allergic, as well as toxic fibrosing alveolitis, the prognosis is usually favorable. As the disease becomes chronic, the prognosis worsens.
Idiopathic fibrosing alveolitis is prone to gradual progression with the development of complications. Due to increasing irreversible changes in the alveolar-capillary system of the lungs, the risk of death is high. The five-year survival rate after surgical treatment reaches 50-60%.