Symptoms
Pericoronitis is accompanied by a number of symptoms.
- Objective symptoms that can be seen by the patient himself or the dentist during an examination of the oral cavity.
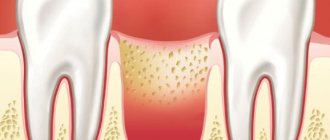
The presence of a mucosal hood on the surface of the erupting tooth and a pathological gingival pocket are determined [6,9,10]. Externally, at the site of the erupting tooth, the gum tissue is hyperemic (red), voluminous due to swelling. The causative tooth may be mobile.
During the examination, the dentist evaluates the regional lymph nodes (cervical, submandibular, preauricular), their size and the presence of pain. An increase in the latter indicates a prolonged course of pericoronitis. With mild severity, the body temperature rises to 37°C, and in the presence of purulent complications - to 38-39°C [2,5,13]. The face with pericoronitis is asymmetrical, due to swelling and enlargement of soft tissues on the affected side.
- Subjective symptoms caused by the patient’s sensations.
Pain in the gums occurs at rest and intensifies when brushing teeth, chewing food, talking and opening the mouth. Pain sensations can spread along the branches of the trigeminal nerve to the ear and eye[7]. There is an unpleasant, putrid odor from the mouth. General health worsens, weakness occurs, sleep is disturbed, appetite and performance decrease. In response to pain, the masticatory muscle spasms, making it difficult to open the mouth, chew and swallow food[11].
Quality and safety
I, the subject of personal data, in accordance with the Federal Law of July 27, 2006 No. 152 “On Personal Data,” provide SCNT “NOVOSTOM” LLC: (hereinafter referred to as the Operator), located at 127030 Moscow, st. Novoslobodskaya, 24, building 4 (checkpoint 770701001), consent to the processing of personal data specified by me in the registration form and/or in the feedback form on the Internet site, owned by the Operator.
The personal data I provide is as follows: full name, email address and telephone number.
The purposes of processing my personal data are: ensuring the exchange of short text messages in online dialogue and ensuring the functioning of a call back.
Consent is provided to carry out the following actions (operations) with the personal data specified in this consent: collection, systematization, accumulation, storage, clarification (updating, changing), use, transfer (provision, access), blocking, deletion, destruction, carried out as with using automation tools (automated processing) and without the use of such tools (non-automated processing).
I understand and agree that providing the Operator with any information about myself that is not contact information and not related to the purposes of this consent, as well as providing information related to state, banking and/or commercial secrets, information about racial and/or nationality, political views, religious or philosophical beliefs, health status, intimate life are prohibited.
If I decide to provide the Operator with any information (any data), I undertake to provide only reliable and up-to-date information and do not have the right to mislead the Operator regarding my identity, or provide false or inaccurate information about myself.
I understand and agree that the Operator does not verify the accuracy of the personal data provided by me and is not able to assess my legal capacity and assumes that I provide reliable personal data and keep such data up to date.
Consent is valid upon achievement of the purposes of processing or in the event of the loss of the need to achieve these purposes, unless otherwise provided by federal law.
Consent may be withdrawn by me at any time based on my written statement.
Types of pericoronitis
Pericoronitis is divided into acute and chronic according to the nature of its course. The first can be catarrhal (mucous discharge predominates), ulcerative (with the formation of erosions and ulcers) and purulent (pus is released) [12,15].
Acute pericoronitis is characterized by:
- rapid start;
- pronounced pain syndrome;
- the presence of discharge from under the gum hood (first serous, then purulent);
Chronic pericoronitis is characterized by:
- sluggish course of the inflammatory process;
- mild symptoms of pain and dysfunction of chewing, swallowing, speech;
- alternating periodic exacerbations and subsidence of symptoms;
- destruction of the cortical plate around the causative tooth and its mobility;
- spread of inflammation to the soft tissues of the pharynx, cheeks, sometimes with the formation of fistulas (canals).
Catarrhal
Catarrhal pericoronoritis is the mildest, initial form of inflammation of the mucous membrane around the erupting tooth [5,9]. This type of disease is characterized by redness of the mucous membrane and swelling of the overhanging edge of the gum. There is no discharge from under the hood between the gum and tooth.
The patient complains of itching of the gums, slight pain in the area of eruption, which may intensify while eating, when touching the affected area of the gums, or closing the jaws. With timely initiation of treatment, acute pericoronitis goes away without a trace [10].
Ulcerative
A characteristic sign of ulcerative pericoronitis is the presence of ulcers on the edges of the hood hanging over the causative tooth. At the site of inflammation, there is an abundant deposition of soft plaque, after removal of which bleeding and gum pain are observed [1,18]. Regional lymph nodes are enlarged, body temperature rises to 37.5°C.
Purulent isolated subacute
The course of purulent pericoronitis is longer than in the acute process, and is therefore classified as subacute. The disease is accompanied by severe pain, which intensifies when chewing, swallowing and speaking, and radiates to the temple and ear. Opening the mouth is difficult and painful [6].
When pressing on the tooth, purulent discharge is released from under the hood of the mucous membrane. A putrid odor appears from the mouth, the patient constantly feels the taste of pus in the mouth[3]. There is enlargement and tenderness of the submandibular lymph nodes. The long course of purulent pericoronitis is accompanied by ulceration of the gums with subsequent scar formation [6,8].
Retromolar periostitis
Inflammation of the periosteum in the area of the last molar of the jaw (wisdom tooth) develops due to purulent pericoronitis and is called retromolar periostitis. The mechanism of development of this disease is associated with the spread of pus under the crown and periosteum of the alveolar process of the jaw, where the wisdom tooth is located [20].
The disease can be suspected if:
- sleep disturbances, including insomnia;
- decreased appetite;
- facial imbalances due to swelling of the painful side;
- decreased functions of the dental system (opening the mouth, chewing, swallowing, speaking);
- temperature rises to 38.5°C.
Treatment of retromolar periostitis is carried out by treatment and excision of non-viable gum tissue, drainage of the purulent focus and complex detoxification therapy (drinking plenty of fluids). In the absence of therapy, purulent melting of the jaw bone tissue, fistula tract and abscess of the soft tissues of the face may develop [17].
Spicy
The acute course of pericoronitis is characterized by a rapid onset, rapid inflammation of the gums near the causative tooth, and severe pain symptoms [15,20]. It develops as a result of complicated tooth eruption, which is caused by its incorrect location in the dental arch or individual structural features of the tissues covering the tooth before its eruption (periosteum, gingival mucosa) [5.9].
The condition for the development of acute pericoronitis is a low oral hygiene index. A direct relationship has been established between the presence of a large amount of dental plaque and the likelihood of developing inflammation of the injured gum mucosa at the time of teething [19].
THE WEBSITE IS UNDER CONSTRUCTION!!!
Teething in children: timing, symptoms, possible complications
At the age of five to six months, a difficult period begins in the life of the child and his parents. Teething syndrome in children is a special physiological condition, which is accompanied by characteristic symptoms : fever , swelling and pain in the gum tissue, loose stools, loss of appetite and other unpleasant symptoms . At this point the child becomes capricious, loses activity, and often cries.
However, some parents, during the period of eruption of the first milk teeth in infants , ignore the baby’s , preferring to simply use painkillers instead of seeking medical advice. Such a mistake can be costly, because by attributing all disorders to a natural physiological process, parents risk ignoring the signal that the child is sick. The process of teething in a baby is a serious reason to go to see a doctor, because it is not for nothing that this syndrome was separately included in the international classification system of diseases ICD 10 , under the index K00.7. Only an experienced and qualified specialist will be able to distinguish the symptoms of the eruption of the first teeth in a six-month-old baby from the manifestations of more serious pathologies that may threaten the child’s health. Professional and timely diagnosis in a medical institution is the only guarantee that treatment of a dangerous disease will begin at an early stage and be successful. And even if there is only a natural physiological stage of the child’s development, the doctor can determine how the process is proceeding and whether any deviations from the norm are observed. And if necessary, an experienced specialist will prescribe effective medications and ointments to relieve teething pain or relieve other symptoms that bother the baby .
Features of the teething process, timing and order of appearance
The statistical norm for the appearance of the first baby teeth in a baby is six months. However, modern medical practice confirms the existence of a tendency to speed up this process. Signs of teething can be observed in children aged five months and, in rare cases, four months. By the first year of life, up to eight incisors can already be observed in a child’s mouth, and by about three years the rest appear. It is worth noting that the dynamics of manifestation and growth depend on many indicators: the sex of the child, heredity, diet, indicator of physical activity, degree of development of organs and systems.
There is no universal data on this issue, but there is a conditional table that reflects the approximate timing and order of teething in children :
- The lower incisors begin to appear very first, this process lasts until nine months of age;
- The upper incisors grow between seven and ten months;
- Lateral incisors from 9 to 12 months, parallel above and below;
- The eruption of the front molars in children will begin from one year to nineteen months, the second ones appear much later - almost at the age of two years;
- The upper canines range from 16-20 months, and the lower ones - up to 22 months.
Symptoms of teething in children and signs of disruption of this process
The first symptom that parents most often pay attention to is fever. Deviations from the norm are usually not too significant - within 37.5 - 38 degrees. It is worth monitoring not only the magnitude, but also the duration. A natural increase in temperature is usually easily relieved with antipyretic drugs. A persistent increase in temperature above 38 indicates that teething syndrome occurs with complications. At this age, the primary immune system is just forming in the child’s body, and inflammatory or even infectious processes can develop in the oral cavity and intestines.
The second important sign that can help the doctor during the eruption of baby teeth is the nature of the mucous discharge. Swelling of the nasal cavity and gums is a natural process during the growth of fangs and incisors of the upper jaw; the mucus is watery in nature. Thick and colored discharge is a sure sign of an ENT disease.
One of the symptoms of teething in babies is also loose stools. In this case, the consistency becomes only slightly thinner than usual. Do not confuse the signs accompanying tooth growth with diarrhea. If a child has a serious intestinal disorder for several days, and eating is accompanied by vomiting, then you should urgently go to the hospital, where an infection will most likely be diagnosed.
But most often, parents turn to doctors with complaints about gum replenishment. Teething is a process in which soft tissue is torn, causing pain . A qualified professional will prescribe topical anesthetics to relieve discomfort and recommend massage techniques to speed up the process. Under no circumstances should you select medications on your own.
Fracture of the tooth crown without damage to the pulp
Symptoms of a tooth crown fracture (tooth enamel fracture, tooth dentin fracture).
Patients diagnosed with a tooth crown fracture without damage to the pulp (tooth enamel fracture, tooth dentin fracture) complain of:
- For short-term pain from any irritant. But the closer the fracture is to the pulp of the tooth, the more intense the pain during a fracture of the tooth crown will be;
- pain when any touch of the tooth;
A doctor in a clinic with a fracture of the crown of a tooth without damage to the pulp (fracture of tooth enamel, fracture of tooth dentin) notes:
- painful percussion;
- pain on probing.
Often, dental trauma such as a fracture of tooth enamel or a fracture of tooth dentin is accompanied by abrasions, hematomas of the lips and cheeks.
Diagnosis of a tooth crown fracture without damage to the pulp (tooth enamel fracture, tooth dentin fracture).
The patient is sent for an x-ray to make sure that there is no fracture of the tooth root and to understand where the fracture line is. Pulp viability tests must be done.
Treatment of tooth crown fracture
Treatment of a fractured tooth crown should be carried out as soon as possible after the injury. Because exposed dentin is a threat to pulp damage. Treatment will consist not only of protecting dentin from the external environment, but also of forming replacement (reparative) dentin. Therefore, it is best to first place a calcium-containing pad on the bottom of the cavity and place a temporary filling. Thus, the doctor warns himself against possible complications, and after the symptoms have been eliminated and a favorable X-ray picture is available, a permanent filling can be placed.
In the next article I will try to talk in detail about complete/incomplete dislocation of a tooth, a fracture of the crown of a tooth with exposure of the pulp, a fracture of the root of a tooth, and we will touch on some features of dental trauma in childhood.
The article was written by N. Shidlovskaya specifically for the OHI-S.COM website. Please, when copying material, do not forget to provide a link to the current page.
Tooth dystopia - symptoms and treatment
One of the mechanisms for the development of dystopia is associated with the abnormal arrangement of tooth germs, which is formed during intrauterine development. The second reason is pathological teething. It is caused by disorders of embryonic development associated with the formation of a tooth germ. They can manifest themselves in the form of macro- and polyodontia, a pronounced disproportion of temporary and permanent teeth.
Another cause of dystopia is genetic characteristics. Sometimes the size of the teeth acquired from one parent does not match the size of the jaws acquired from the other parent. This discrepancy can lead to crowding of the teeth or the appearance of spaces between them, which can further contribute to the development of dystopic teeth.
Exogenous factors of dystopia, as a rule, are traumatic in nature. These include scarring on the gums, mechanical damage to the teeth and bad habits such as thumb sucking or biting a pen or pencil. For example, with prolonged thumb sucking, the incisors of the upper jaw change the direction of growth, thereby forming an open bite.
Also, the development of dystopia is provoked by partial adentia, premature removal of baby teeth, and violation of the timing and sequence of eruption.
Late teething is promoted by:
- damage to dental follicles due to trauma or infection in the area of primary teeth;
- development of a benign tumor and odontogenic cyst;
- anomalies in the size and shape of adjacent teeth;
- excessive retention of baby teeth in the socket;
- impaired jaw growth after injuries, endocrine disorders, rickets, vitamin deficiency and hypovitaminosis [5].
The effect of the endocrine glands on metabolic processes and the formation of the dental system begins in intrauterine development. For example, children born to mothers with toxic goiter (autoimmune disease of the thyroid gland) experience intrauterine eruption of primary teeth, a delay in the appearance of permanent teeth, early mineralization of the crowns and formation of the roots of permanent teeth.
Against the background of acquired hypothyroidism, the rate of eruption of milk and permanent teeth slows down. Teeth of atypical shape appear, some elements rotate around their axis or begin to grow outside the dental arch.
With rickets, the growing body lacks vitamin D. As a result, the exchange of phosphorus and calcium, which play an important role in the formation of jaws and teeth, is disrupted. This causes the jaw bones to become underdeveloped, narrowed, or flattened, preventing teeth from growing and functioning properly. In these cases, they pile up on top of each other, that is, they crowd together.
An excess of vitamin A causes abnormal growth of the jaws, tongue and dentin density. With a lack of vitamins A and B, atrophy of the salivary glands may develop, which leads to changes in the periodontium. With a lack of phosphorus against the background of normal levels of calcium and vitamin D, jaw growth and teething slow down, which subsequently leads to dystopia and malocclusion.