From this article you will learn:
- symptoms of lymphadenitis in children and adults,
- reasons for the development of inflammation,
- acute and chronic lymphadenitis - treatment, antibiotics.
The article was written by a doctor with experience in maxillofacial surgery.
Lymphadenitis is an inflammation of one or more lymph nodes that occurs against the background of acute or chronic infection. Most often, lymphadenitis occurs in children (due to the imperfection of their immune system), and at an outpatient appointment with a pediatric dentist, lymphadenitis is diagnosed in approximately 5-7% of all children. Moreover, lymphadenitis in children under 5 years of age occurs primarily due to acute respiratory viral infections, infectious processes in the tonsils, inner and middle ear, and in children after 6-7 years of age - due to foci of purulent inflammation at the roots of the teeth.
In approximately 40% of cases, inflammation of the lymph nodes is not diagnosed in time. This is due to the fact that pediatricians and pediatric dentists, to whom parents most often bring their children for examinations, do not have much experience in working with this pathology. As for adults, lymphadenitis occurs in them much less frequently than in children, and its development is usually caused by a combination of factors - the presence of acute or chronic purulent inflammation + a weakened immune system.
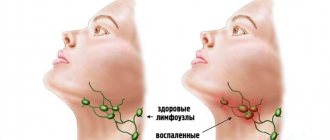
Lymphadenitis: photo
There are many groups of lymph nodes on the face and neck, the main ones being the buccal, parotid, submandibular (submandibular), retromandibular, submental, retropharyngeal, as well as superficial and deep cervical lymph nodes. In healthy children and adults, the lymph nodes are never enlarged, but if they are enlarged, this almost always happens as a result of invasion of pathogenic microorganisms. But we must remember that in some cases, enlarged lymph nodes may indicate tumor growth or blood diseases.
Structure and function of lymph nodes –
In the body, lymph nodes play the role of a biological filter. Lymph nodes retain and destroy pathogenic bacteria and toxins that enter them through lymphatic vessels - from teeth and bones affected by inflammation, tonsils, soft tissues of the face, and other organs and tissues. However, with the constant chronic sedimentation of microorganisms in them, they lose the ability to neutralize them, and in some cases they themselves turn into sources of purulent infection.
Each lymph node has a connective tissue capsule on the outside, from which lymphatic vessels depart, providing inflow or outflow of lymph. Thin connective tissue septa (trabeculae) extend from the capsule into the lymph node, between which the parenchyma is located. Closer to the capsule, the parenchyma consists of lymphoid follicles, and closer to the center of the lymph node - of strands of lymphocytes. The lymph passing through the lymph node is cleared of infectious agents and other antigens, and the so-called “immune memory” is also formed here.
Inflammation of the lymph nodes in the neck: causes
As we said above, different causes of lymphadenitis prevail at different ages. In children under 5 years of age, the main role is played by acute respiratory viral infections (influenza, pneumonia, tonsillitis, otitis, rhinitis), as well as foci of chronic infection in the tonsils, inner and middle ears. Less commonly, the development of lymphadenitis at this age is associated with pustular lesions of the skin of the face and head, as well as with inflammation of the oral mucosa due to stomatitis or as a result of traumatic damage. The development of lymphadenitis can also be triggered by the BCG vaccine against tuberculosis.
Diagnosis and treatment of all of the above non-odontogenic lymphadenitis (i.e., not associated with teeth) is most often carried out by pediatricians and infectious disease specialists. But as for the age from 6 to 12 years, up to 70% of cases of inflammation of the lymph nodes in a child are associated with foci of purulent inflammation in the area of the roots of the teeth. Lymphadenitis, the cause of which is inflammation of the teeth, is called “odontogenic”. And therefore, the first doctor you should contact in order to find the source of the infection should be a dental surgeon.
Causes of odontogenic lymphadenitis in children and adults –
- acute purulent periodontitis (or exacerbation of chronic periodontitis),
- suppuration of a cyst at the apex of the tooth root,
- difficult teething (including the lower wisdom tooth),
- alveolitis (inflammation of the socket of an extracted tooth),
- purulent periostitis (flux),
- osteomyelitis of the jaws,
- perimaxillary abscesses and phlegmons,
- odontogenic sinusitis,
- stomatitis of the oral mucosa.
Differences between odontogenic and non-odontogenic lymphadenitis –
As for odontogenic lymphadenitis, most often complaints are made about unilateral inflammation of the lymph nodes in the neck, which corresponds to the submandibular group of lymph nodes (submandibular lymphadenitis). If you start questioning the patient, you can often find that inflammation of the lymph node was preceded by pain in one of the teeth, or gumboil may have formed on the gum before this, or one of the teeth was recently treated by a dentist. Those. usually there is always an exact connection between inflammation of the lymph node and the causative tooth (on the same side), or with a disease of the oral mucosa.
In acute nonodontogenic lymphadenitis, patients complain of the appearance of not one, but usually several “balls” at once in the submandibular region or upper parts of the neck. Moreover, patients clearly associate this with a recent sore throat, otitis media or acute respiratory viral infection. A feature of non-odontogenic lymphadenitis is that inflammation of the lymph nodes occurs in several anatomical areas at once, often symmetrical (by the way, this is one of the distinctive signs of non-odontogenic lymphadenitis). In addition, non-odontogenic lymphadenitis is always accompanied by a general inflammatory process in the body associated with the underlying disease, for example, otitis media or tonsillitis.
Which lymph nodes are most likely to become inflamed?
Moreover, it is approximately always possible to determine the source of inflammation of a lymph node if you know the paths of lymph outflow from various areas of the face - to the lymph nodes of a certain location. Most often in children and adults, inflammation of the submandibular lymph nodes located along the lower edge of the lower jaw occurs. Lymph flows into the submandibular nodes from the bone tissue, periosteum and teeth of the lower jaw (from the canine to the third molar), as well as from the tonsils, skin of the external nose and the anterior mucous membrane of the nasal cavity.
In addition, lymph partially enters the submandibular lymph nodes from bone tissue, periosteum and teeth of the upper jaw (from the fourth premolar to the third molar). An important point is that slightly deeper than the submandibular lymph nodes there are retropharyngeal lymph nodes, to which lymph flows from the middle ear, from the posterior parts of the nasal cavity, and also partially from the tonsils, and from the hard and soft palate.
Another important group is the mental lymph nodes, into which lymph flows from the skin of the upper and lower lips, from the roots of the lower incisors and canines, from the bone and periosteum of the mental region of the lower jaw. Accordingly, inflammation of this group by the lymph node can be caused, for example, by a focus of purulent inflammation in one of the lower front teeth. But lymph flows to the parotid lymph nodes from the skin of the forehead, ears, external auditory canals, cheeks and upper lip. Accordingly, inflammation of the parotid lymph nodes can be triggered by an inflammatory process in these tissues.
Oncological alertness
Lymph nodes are often enlarged due to lymphogranulomatosis (Hodgkin's lymphoma) or lymphosarcoma (non-Hodgkin's lymphoma). These are malignant processes that are manifested by increased density, painlessness and large diameter of the lymph nodes in the absence of other reasons for their deformation. Lymph nodes enlarge in groups, asymmetrically (for example, on one side of the neck). At the initial stage of the process, their mobility and separate arrangement are maintained. If the oncological process continues without treatment, the lymph nodes may become fused, and moderate pain rarely occurs. Source: N.V. Nagornaya, E.V. Vilchevskaya, A.P. Luachak, E.N. Marchenko, E.V. Bordyugova, A.P. Koval Hodgkin's disease (lymphogranulomatosis) in children // Child's Health, 2013, No. 1 (44), pp. 13-15
Symptoms that require consultation with a doctor are enlarged lymph nodes:
- more than 7 days;
- more than 1 group;
- accompanied by elevated body temperature;
- in a child under one year old;
- progressive over time;
- with changes in local skin.
Classification of lymphadenitis –
There are several classification options for lymphadenitis. For example, according to the localization of inflammation, lymphadenitis can be submandibular, submental, retromandibular, parotid, cervical, etc. According to the route of infection, lymphadenitis is divided into – 1) “odontogenic”, i.e. in this case, the infection is associated with the teeth, 2) “non-odontogenic”, i.e. associated with a viral or bacterial infectious process of a non-dental nature (this may include sepsis or a specific infection such as tuberculosis, syphilis, actinomycosis, AIDS).
The most important classification takes into account the severity of the inflammatory process and divides lymphadenitis into acute and chronic. In turn, acute lymphadenitis can be serous and purulent. It must be said that acute serous lymphadenitis, in which there is still no focus of purulent inflammation in the tissue of the lymph node (and there is only serous infiltration), is the only form of lymphadenitis that can be treated conservatively without surgical intervention. But very often patients go to the doctor too late, when foci of necrosis form in the tissues of the lymph node and a cavity with pus forms.
As for the chronic forms of lymphadenitis, there are hyperplastic, purulent and aggravated chronic. In the chronic hyperplastic form, there is a slow, constant increase in the volume of the lymph node (due to the replacement of lymphoid tissue - connective tissue). However, in the case when, against the background of weakened immunity or high virulence of the infection, inflammation spreads beyond the border of the lymph node capsule, adenophlegmon can form. It should be noted that each of the acute and chronic forms is characterized by its own special symptoms.
Acute and chronic lymphadenitis: symptoms
Lymphadenitis is characterized by a certain seasonality of the disease - most often it occurs in the autumn-winter period and early spring. In the first case, the outbreak is explained primarily by the active state of the immune system during this period, and an overreaction to any infection. In the spring, on the contrary, it is associated with the weakness of the immune system and the inability of the lymph nodes to resist a large volume of pathogenic microorganisms. So, let's move on to the symptoms of different forms of lymphadenitis...
1) Acute serous lymphadenitis - it is characterized by an enlargement of the lymph node (sometimes quite significant), as well as the appearance of pain. The general condition is satisfactory, the temperature is usually not higher than 37.5, there are no changes in the blood and urine. Upon palpation, an enlarged painful node is felt, usually round in shape, the skin is not fused to it (i.e., the skin above the lymph node gathers in a fold), and its color is not changed. As the inflammation subsides, the lymph node shrinks, gradually becomes softer, and the pain disappears (24stoma.ru).
2) Acute purulent lymphadenitis - if a child does not have an appointment with a dental surgeon or pediatrician for 5-7 days, then serous inflammation usually turns into purulent inflammation. This is also facilitated by active home self-medication in the form of various compresses and warming up. The rapid transition of serous inflammation into purulent inflammation is facilitated by an incorrect diagnosis by pediatricians, who immediately prescribe heat compresses, thereby accelerating the transformation of serous inflammation into purulent inflammation (as a result of which such children quickly end up in the maxillofacial department).
In acute purulent lymphadenitis, complaints are usually made about an enlarged lymph node, in which throbbing pain appears, a significant increase in body temperature up to 38.0 ° C, loss of appetite (in children this causes a change in behavior, the child becomes capricious and restless). In the projection of the inflamed lymph node, tissue swelling appears, and upon palpation a painful round-shaped infiltrate is felt. The skin in the projection of the lymph node becomes red and gradually fuses with the lymph node (i.e., it will not gather into a fold). Over time, a focus of softening may appear in the center of the infiltrate, i.e. symptom of fluctuation.
If the inflammation is localized in the retropharyngeal or parotid lymph nodes, then swallowing is usually painful, and mouth opening is most often limited. As for adults, their symptoms can occur in the same way as described above, but can often be erased. In the latter case, the formation of a purulent abscess inside the lymph node occurs slowly (sometimes within 2-3 weeks), and is not accompanied by severe general and local symptoms. Lack of treatment for acute purulent lymphadenitis can lead to pus leaving the capsule of the lymph node, i.e. into the surrounding tissues, and the development of a serious complication - adenophlegmon.
3) Chronic hyperplastic lymphadenitis - this form of lymphadenitis occurs mainly only in adults, it develops slowly (sometimes over 1-2 months or even more). Patients usually complain of the presence of some kind of round formation in the soft tissues, and sometimes also of weakness and malaise. The general condition is usually satisfactory, and only in the evening the temperature can rise to 37-37.5 °C. Initially, a painless or slightly painful pea appears deep in the tissues of the face or neck, which gradually enlarges and thickens.
On palpation, a round-shaped lymph node is palpable, with clear contours, mobile and not fused to the underlying tissues. Sometimes a significant proliferation of granulation tissue occurs in the lymph node, which extends beyond the lymph node capsule and grows to the skin, thinning it. When thinned skin breaks through, a fistulous tract usually forms, from which granulations bulge. This form of lymphadenitis can periodically worsen, and then during the period of exacerbation the symptoms will correspond to acute purulent lymphadenitis.
4) Chronic purulent lymphadenitis - this chronic form of lymphadenitis occurs in both children and adults. Patients usually complain of a long-term “ball” (usually in the submental or submandibular area), which does not cause any particular inconvenience. From a survey, you can usually find out that the ball first appeared several weeks or months ago - most often after pain in a tooth on the side of the inflamed lymph node. Subsequently, the pain in the tooth disappeared, but the slightly enlarged lymph node remained.
Patients may also note that over the course of several months there have been one or more cases of exacerbation of chronic inflammation, which was manifested by a slight increase in temperature, an increase in the size of the lymph node and its soreness. In this case, upon palpation, a dense, painful, limitedly mobile, round-shaped formation not fused to the skin is felt, in the center of which a focus of softening (fluctuation) can be detected.
5) Adenophlegmon - occurs when the lymph node capsule melts, when the pus contained in it penetrates into the surrounding loose tissue. Those. diffuse purulent inflammation occurs. Patients usually complain of intense, spontaneously occurring pain in any area, as well as deterioration in health, chills, and an increase in body temperature to 38-38.5 °C. In rare cases, adenophlegmons develop slowly, the symptoms are erased, and the body temperature does not exceed 37.5-38 °C.
Patients always usually say that the disease began with the appearance of a painful ball (pea), gradually increasing in size. Over time, a diffuse infiltrate appeared in the tissues, the skin on which became red and gradually stopped folding. The release of pus from the lymph node into the surrounding tissue is accompanied by an increase in the area of the infiltrate, the skin gradually becomes purple, and a focus of softening may appear in the center of the infiltrate. Treatment of adenophlegmon is only surgical; an urgent autopsy is indicated, and the location of the external incisions will depend on the location of the inflammation.
Establishing diagnosis -
Diagnosis of odontogenic lymphadenitis is quite simple, because There is always a connection with toothache and gum inflammation. When examining the teeth in this case, you can find either a destroyed tooth, or a tooth under a filling or crown. Biting on such a tooth can be painful, or there was pain in it quite recently. There may be a fistula or lump on the gum in the projection of the causative tooth, and pressing on the gum can be painful. If the inflammation in the dental area is chronic and almost asymptomatic, then panoramic radiography will help us.
It can be more difficult to make a correct diagnosis with non-odontogenic lymphadenitis, which in this case must be distinguished from an abscess, phlegmon, sialadenitis, salivary stone disease, suppurating atheroma, as well as from specific lymphadenitis in syphilis, tuberculosis and actinomycosis. In acute forms of lymphadenitis, puncture plays a decisive role in making the correct diagnosis. Examination of punctate allows you to make a correct diagnosis and distinguish ordinary nonspecific infectious lymphadenitis from specific lesions (actinomycosis, tuberculosis, syphilis, as well as oncology).
In addition, chronic hyperplastic lymphadenitis must be distinguished from congenital cysts and fistulas of the face and neck, tumors, as well as from lymphogranulomatosis (puncture will also help us here). It is equally important to pay attention to other lymph nodes during the examination, because an increase in several groups of facial and cervical lymph nodes at once should alert you to certain blood diseases and HIV infection.
General information
The organs of the lymphatic system play a protective role in the human body. They serve as a barrier to viruses, bacteria, and also filter out harmful substances. In total, there are more than 450 lymph nodes in the adult body, and their maximum number is formed by the age of 10.
Lymph nodes are connected by lymphatic vessels - lymph (a fluid with a high content of lymphocytes, or “white blood cells”) circulates through them. Produced in the bone marrow, lymphocytes circulate throughout the body, first passing through the spleen and then the lymph nodes. Thanks to this, they gain the ability to produce antibodies to destroy microbes. Source: A.G. Rumyantsev, professor, V.M. Chernov, professor, V.M. Delyagin, professor Enlarged lymph node syndrome as a pediatric problem Practical Medicine, 2007, No. 5 (24), pp. 12-15
When an infection enters , a kind of “attack” is carried out on it, as a result of which the lymph nodes can enlarge (during this period they more actively produce antibodies). After recovery, the nodes return to normal size. If their diameter and density do not return to their original state, the child must be shown to a doctor.
Lymphadenitis: treatment
In the treatment of lymphadenitis, the main thing is to eliminate the cause of its occurrence.
Accordingly, in case of odontogenic lymphadenitis, depending on the condition of the tooth and the age of the child, it is necessary to treat or remove the causative tooth. If in adults it is desirable to preserve a tooth in all possible cases, then in children the situation is much more complicated. In children, inflammation at the root apex is treated only in permanent teeth; baby teeth must be removed. This is due to the wide root canals of baby teeth, the immaturity of the apexes of the roots of baby teeth, on which huge apical foramina gape. Such teeth cannot be properly filled, plus there is too great a risk of injury to the permanent tooth germ. Numerous attempts to treat such teeth end in almost 100% of cases with complications - the development of purulent periostitis, inflammation and loss of the permanent tooth germ, sometimes with sepsis and even death. And this is not to mention the fact that the long-term presence of a focus of purulent inflammation in a child affects the entire body, suppresses its immunity, contributing to the occurrence of frequent infectious diseases, allergic reactions, bronchial asthma and other pathologies. This is worth remembering when a not very competent doctor suggests not removing such a tooth, citing possible problems with the bite in the future.
Accordingly, if it is possible to save a permanent tooth in a child or an adult, the tooth is opened (removal of carious tissue, old filling or crown, revision of the root canals) to create an outflow of pus through the root canal. Next, general therapy is prescribed, and after the cessation of suppuration, the inflammatory focus at the apex of the tooth root is treated in the standard way, as for chronic periodontitis, i.e. with placing a special medicinal paste into the root canals. All these actions will prevent further transmission of infection from the source of inflammation - to the lymph nodes.
1) Treatment of serous lymphadenitis -
The treatment tactics for serous lymphadenitis will depend on what day after the onset of the disease the patient went to the doctor (the earlier, the greater the chance of success of conservative treatment). In this case, conservative treatment is first used - compresses with a 5% solution of dimexide, in which anti-inflammatory medications are dissolved. To do this, add 1 ml of hydrocortisone solution, 50% analgin solution and 1% diphenhydramine solution to 10 ml of a 5% dimexide solution.
Drug Dimexide (99% concentrate) –
Next, apply a classic compress to the area where the affected lymph node is located. A gauze cloth is generously moistened with the solution, and a plastic film is placed on top of it (to isolate the solution from air). Under no circumstances should you make a thermal compress by placing any material or towel over the film. Thermal procedures, if this is not 1-2 days of development of the disease, will only aggravate congestion in the lymph node and will contribute to the development of pathogenic microorganisms, i.e. the transition of serous inflammation to purulent (for the same reason, you should not do UHF, bandages with Vishnevsky ointment).
If a child or adult consults a doctor in the first 2-3 days from the onset of the disease, the most effective is the use of physiotherapy methods - phonophoresis of hydrocortisone, electrophoresis of dimexide with an antibiotic and diphenhydramine, laser therapy.
2) Treatment of purulent forms of lymphadenitis -
Surgery is used to treat acute purulent lymphadenitis, exacerbation of chronic purulent lymphadenitis, adenophlegmon. The operation is performed in a hospital setting under general anesthesia, and it is necessary to scrape the necrotic tissue of the lymph node from the wound. In case of chronic hyperplastic lymphadenitis, it is better to remove the lymph node followed by histological examination (moreover, if there is a fistulous tract with granulations growing to the surface of the skin, the lymph node is removed along with the fistulous tract).
After opening the abscess, physiotherapy is prescribed - enzyme electrophoresis, UHF, magnetic therapy, helium-neon irradiation, ultraviolet radiation. Depending on the severity of inflammation, intoxication and the state of immunity, various medications are used. First of all, these are detoxification and antihistamines, sometimes antibiotics. For inflammation of the lymph nodes, not just any antibiotics are used, but those that tend to accumulate in the lymph nodes, for example, the combination of ampicillin + sulbactam, cefazolin, claforan).
Removal of a lymph node for hyperplastic lymphadenitis –
Diagnostic methods
After examination and collection of complaints and medical history, the specialist sends the child for a general examination . It includes x-rays, blood and urine tests . Additionally, the following studies may be needed:
- blood serology;
- diagnosis of tuberculosis;
- lymph node biopsy followed by cytological examination in the laboratory;
- Ultrasound.
Sometimes children are prescribed antibacterial drugs as part of the diagnosis. Based on their effectiveness, they confirm or refute the bacterial nature of the disease.
Complications of lymphadenitis –
As for complications, lymphadenitis can be complicated by adenophlegmon, and the latter can lead to the development of phlebitis, thrombophlebitis, and sepsis. The causes of complications are usually:
- a sharp weakening of the immune system due to viral and infectious diseases,
- if in the source of inflammation, in addition to the usual microflora (staphylococcus, streptococcus), there are also anaerobes (for example, clostridia and fusobacteria),
- errors in diagnosis,
- untimely start of treatment,
- improper treatment, including attempts at home self-medication.
Prevention of lymphadenitis is timely sanitation of the oral cavity, as well as foci of acute and chronic infection in the body. We hope that our article: How to treat neck lymphadenitis was useful to you!
Sources:
1. Higher medical education of the author of the article, 2. Based on personal experience in maxillofacial surgery and dental surgery, 3. National Library of Medicine (USA), 4. The National Center for Biotechnology Information (USA), 5. “Outpatient surgical dentistry" (Bezrukov V.), 6. "Pediatric surgical dentistry and maxillofacial surgery" (Topolnitsky O.).
Prices
| Name of service (price list incomplete) | Price |
| Appointment (examination, consultation) with an allergist-immunologist, primary, therapeutic and diagnostic, outpatient | 1750 rub. |
| Consultation (interpretation) with analyzes from third parties | 2250 rub. |
| Prescription of treatment regimen (for up to 1 month) | 1800 rub. |
| Prescription of treatment regimen (for a period of 1 month) | 2700 rub. |
| Consultation with a candidate of medical sciences | 2500 rub. |
| Allergen-specific immunotherapy (ASIT) - maintenance course (excluding the cost of the drug) | 8100 rub. |