Chronic apical periodontitis
Chronic apical periodontitis is most often an asymptomatic inflammation in the tissues of the apical periodontium, which is manifested by radiological changes at the apex of the tooth roots.
Many dentists use the clinically convenient classification of I. G. Lukomsky. It simplifies the diagnosis.
Chronic fibrous periodontitis
Occurs as an outcome of acute periodontitis or treatment of granulating and granulomatous periodontitis. Traumatic etiology is also important due to overload, which occurs with the loss of a large number of teeth or non-physiological articulation.
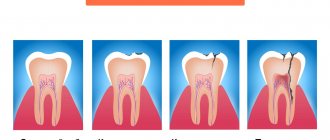
Chronic fibrous periodontitis is detected on an x-ray as an expansion of the periodontal fissure in the apex area and is almost never accompanied by destruction of the adjacent bone.
Chronic granulating periodontitis
It is the most active form among all chronic periodontitis and is the outcome of an acute process.
The patient complains of unpleasant, slightly painful sensations when biting on the causative tooth.
Externally, the patient looks as usual, sometimes there is an increase in the submandibular lymph nodes. In the oral cavity we see hyperemic mucosa in the tooth area, painful on palpation. A distinctive feature of this type of periodontitis is the presence of a fistula in the projection of the root apex. It may ooze pus or bulge granulations. Young granulation tissue grows through damaged cement or even dentin into the bone marrow spaces, often growing along the walls of the fistula tract. The tooth is destroyed or intact. Percussion is weakly positive.
On the x-ray we see a clearing area due to bone destruction in the area of the root apex. The lesion has unclear contours and comes in different sizes.
Chronic granulomatous periodontitis
This type of periodontitis is asymptomatic and manifests itself clinically only during exacerbations. These manifestations can be of the type of granulating periodontitis in the form of fistulas and hyperemia of the mucous membrane.
The difference between granulomatous periodontitis and granulating periodontitis is the presence on the radiograph of a clearing focus at the apexes of the roots with a clear round shape (apical granuloma).
Currently, doctors are moving away from grading the size of the lesion (0.5 cm - granuloma, 0.6-0.8 cm - cystogranuloma, more than 0.8 cm - radicular cyst.
Price
The cost of periodontitis treatment is always strictly individual and consists of a combination of factors. These include diagnostics at the initial and intermediate stages of treatment, the diagnosis made and the algorithm of treatment measures adopted on its basis, the number of visits, drugs, equipment and technologies used in treatment, the work of specialized specialists if necessary, the level of qualifications of the doctor.
Periodontitis is a very serious disease of the teeth and the dental system as a whole. Failure to consult a doctor in a timely manner and attempts at self-medication can lead to serious complications, including those that can threaten your life. At the first appearance of symptoms, you must urgently visit the dental clinic! Be prepared for long-term treatment, which involves multiple visits to the doctor, since the treatment of periodontitis consists of several stages, each of which cannot be started without diagnostically proven effectiveness of the previous one. Only this approach to treatment, combined with the professionalism of the doctor and the patient’s strict, vigilant attitude to all prescriptions and recommendations, is a guarantee of high-quality treatment and reliable protection against relapse for several years.
According to antiplagiat.ru, the uniqueness of the text as of October 16, 2018 is 99%.
Key words, tags: caries, pulpitis, bone tissue destruction, cyst, odontogenic cyst, flux, OPTG image, tooth-preserving operations, resection of the apex of the tooth root, cystectomy, root amputation, dental microscope, preservation, tooth extraction .
1 I. Zimin “From the history of dentistry.” 2 “Teeth and dentistry. Essays on history” / K.A. Pashkov. – M.: Veche, 2014. – 240 p.: ill. 3 Britova, A. A. Endodontics. Diseases of the dental pulp and periapical tissues: textbook. manual, 3rd ed., rev. and additional / A. A. Britova; NovSU named after. Yaroslav the Wise. – Veliky Novgorod, 2016. – 171 p. 4 https://elestom.ru/recommends INTERNATIONAL CLASSIFICATION OF DENTAL DISEASES ICD-C-3 BASED ON ICD-10. 5 https://elestom.ru/recommends INTERNATIONAL CLASSIFICATION OF DENTAL DISEASES ICD-C-3 BASED ON ICD-10. 6 https://mkb-10.com 7 Kleshchenko A. V. Improving the technique of unfilling root canals of teeth obturated with gutta-percha: Dissertation of a candidate of medical sciences: 01/14/14 / Kleshchenko Alexander Viktorovich; (Place of defense: Moscow State Medical and Dental University). - Moscow, 2011 - 93 p. 8 Report of the American Society of Microbiology based on the work. Author: Tobjörn Bengtson, presented by the Faculty of Clinical Medicine, School of Health Sciences, Örebro University, Sweden. * NOS is an abbreviation for “not otherwise specified,” meaning “unspecified” or “unspecified.”
Cyst - what is it and why?
A cyst is a cavity that has an epithelial lining and cystic contents. There are two types of cysts - true and pocket.
The true one is completely covered by the epithelial lining, and the pocket one communicates with the root canal, it seems to grow from it.
Cyst formation occurs in 3 stages.
At the first stage, the epithelial cells of the islets of Malasse most likely proliferate under the influence of growth factors.
During the second stage, an epithelial cavity is formed.
These epithelial cells are directed away from their source of nutrition, die, and neutrophils drag their remains into the area of necrosis. Microcavities are formed, which then merge into one and become limited by stratified squamous epithelium.
There is another theory - the theory that the epithelium covers all open connective tissue areas, resulting in necrosis.
At the third stage of cyst formation after the death of neutrophils, there are reserves of prostaglandins, as well as cytokines produced by macrophages and T lymphocytes. Together they activate osteoclasts and trigger bone resorption.
Pocket cysts have a different mechanism of development. There is a large accumulation of neutrophils near the apical foramen in response to root canal infection. The cells die, as before, and this microabscess is closed by proliferating epithelium. A so-called epithelial ring is formed. Neutrophils that remain outside the channel die and form a microcavity. The presence of infection outside the canal further attracts neutrophils, expanding the microcavity to larger sizes. A pocket cyst is called such because the enlargement of the root canal resembles an enlargement of the periodontal pocket.
Traumatic periodontitis
Periodontal trauma is one of the initiating factors in the occurrence of hemorrhage and the development of ischemia, which directly leads to the formation of pulp necrosis. The focus of necrosis attracts bacteria, colonizes them and infects the periodontium. With an increase in the number of microorganisms, acute inflammation begins. Traumatic periodontitis develops.
With chronic long-term trauma, periodontal restructuring occurs gradually, first due to its adaptation, then as chronic inflammation with lacunar resorption of the compact lamina.
The main reason for the development of pathology is the inflammatory response. As a result of occlusal trauma, inflammatory mediators are produced in the pulp; they are considered a protective reaction to mechanical aggression. They disrupt microcirculation and increase vascular permeability. The pulp dies.
When pulp necrosis reaches the apical periodontium, due to its cytotoxic effect, interleukins activate osteoclasts and bone resorption.
Periodontal anatomy
The periodontium (from Latin perio - around, around; odontos - tooth) is a complex of tissues surrounding the tooth and holding it in the socket. It includes the gum, dental cement, alveolar bone, periodontal ligament, which is located between the dental root and the alveolar plate and communicates between the alveolar bone and the cement of the tooth root. The periodontium consists of many blood and lymphatic vessels, nerve endings, and periodontal fibers. The thickness of periodontal fibers depends on age and averages 0.2 mm, becoming thinner over the years. The periodontal ligamentous apparatus is represented by groups (bundles) of fibers that have different directions, connecting all areas of the periodontium into a single system, stretching between the teeth, from the cement of one tooth to the cement of another. The ground substance of the periodontium occupies about 60% and is an amorphous gel-like substance, 70% consisting of water. A large amount of base material and water in it are factors that play a huge role in providing shock absorption. A characteristic feature of the cellular structure of periodontal tissue is the ability for rapid renewal, but with age this process becomes slower. The structural integrity of the periodontium is ensured by the enamel attachment, the cells of which are completely renewed within 4–8 days. This ability to renew provides mechanical protection of the entrance to the marginal part of the periodontium and reduces the risk of negative factors affecting it. The periodontium performs the most important functions. Plastic – ensures the growth and development of teeth due to the activity of osteoblasts and cementoblasts; trophic – provides nutrition to the cement base of the tooth and the alveolar plate; supporting-retaining – ensures fixation of the tooth in the alveolus; shock-absorbing - distributes chewing pressure due to the ligamentous apparatus; protective – prevents the entry of pathogenic microorganisms and the spread of inflammatory processes 3.
Medicinal periodontitis
Drug-induced periodontitis develops when aggressive liquids or drugs, such as arsenic paste, formalin, tri-cresol formalin, and phenol, enter the periodontium. Penetration into the periodontium occurs through the root canal.
This also includes periodontitis, which develops in response to the removal of phosphate cement, resorcinol-formalin paste, pins and other filling materials into the periodontium during the treatment of pulpitis. Drug-induced periodontitis also includes periodontitis due to allergies as a result of the use of drugs that can cause a local immune response (antibiotics, eugenol, etc.).
Treatment methods
Treatment of periodontitis is a very long process that requires several visits to the dentist and x-ray control at all stages. The essence comes down to clearing the canals from the source of infection and placing the drug inside the tooth, installing a temporary filling - this procedure is repeated several times until the inflammatory process is completely stopped. At the same time, drug therapy is prescribed. Next, the canals are filled and, if necessary, an inlay or crown is installed to restore the apex of the tooth.
Treatment of dental canals In case of periodontitis, as in pulpitis, a thorough cleaning of the dental canals is carried out - endodontic treatment. But if in case of pulpitis the cavity can be filled almost immediately, then in case of periodontitis anti-inflammatory and antibacterial drugs are injected into the canals, more than once. The process is controlled by x-ray examination. Only after the source of inflammation has been completely eliminated can the canals be filled. The cost of treatment directly depends on the number of roots of the tooth.
Price:
from 8,500 rubles more about the solution
Installation of a core inlay If the tooth crown is severely damaged and it is impossible to place a classic composite filling, you will need to build up the tooth and at the same time strengthen its root. One of the best options is to install a stump tab. It differs from a pin in that it is created strictly individually, that is, it completely replicates the structure of the root system of the tooth. Afterwards, you can build up the top with composites or install a crown.
Price:
from 5,000 rubles more about the solution
Installing a crown It may be necessary to place a crown on a tooth if its top is severely damaged. But first, most likely, the tooth will need to be strengthened, because an artificial crown requires some kind of foundation. The prosthesis can be made of various materials: metal-ceramics for the sides, solid ceramics for the front, or zirconium dioxide for any group of teeth.
Price:
from 11,000 rubles more about the solution
Foreign bodies
Gutta-percha, paper pins, calcium residues and a wide variety of other things can be found in the periapical tissues.
The apical periodontium always reacts to foreign bodies. They can enter through the root canal, through an injured mucous membrane or periodontal pocket.
In the case of paper pin penetration, it should be remembered that the human body does not know how to process cellulose, so the foreign body is surrounded by a bacterial plaque, which maintains inflammation.
Gutta-percha is a biocompatible material. However, at the same time it can give a reaction from the apical periodontium. Studies in guinea pigs have shown that large particles of gutta-percha are encapsulated and surrounded by collagen fibers, while small particles support a local tissue reaction. And magnesium and silicon, which are contained in excess gutta-percha, can cause resorption.
Historical reference
Periodontitis, as a concept, did not previously exist, but, of course, this disease has worried humanity, and its history dates back more than one millennium. Thus, in the scientific literature there has been a discussion for a very long time about the methods of dental treatment in Ancient Egypt. The basis for the debate is a number of artifacts, which indicate the predominance of conservative treatment methods in dentistry of that time, and no traces of surgical intervention were identified during the study of the mummies of the pharaohs1. At the same time, a study of mummies showed that the ancient Egyptians suffered from severe damage to the teeth and periosteum, from which we can conclude that periodontitis “flourished” among the first persons of Ancient Egypt, along with other dental diseases. Egyptologist M.A. Raffer wrote that in Egyptian cemeteries it was not uncommon to find diseased teeth that had almost fallen out of inflamed sockets, or carious teeth that were the cause of extensive diseases of the jaws, which could have been avoided and/or cured by performing simple operations 1.
In general, the existence of these dental artifacts inexorably indicates that such a pathology of the dental system as periodontitis has existed for more than one century. But in those days, the symptoms by which today medical science classifies and treats this disease were symptoms of simply a “sick tooth.”
More than a century and a half later, in 1889, a Swiss mechanic and formerly an experienced watchmaker, August Maillefer, who was seriously interested in dentistry, together with his three sons founded a company that was engaged in the creation of high-precision mechanical instruments and gave it his family name - Maillefer. Maillefer used his extensive experience working with watch movements, characterized by unsurpassed “Swiss” precision, to expand the capabilities of dentistry.
Perhaps the first serious treatise, which described about 130 dental diseases caused by various reasons, was the work “The Dentist-Surgeon, or Treatise on Teeth” by P. Fauchard, published in 1728. He also became the author of a number of new filling materials and dental instruments 2. As if anticipating the role endodontic instruments would play in the future, the Maillefer company was the first in the world to invent trimers, pulp extractors, files - tools for working in dental canals. Since 1995, this company became part of the DENTSPLY concern, later called DENTSPLY IMPLANTS, and today it is DENTSPLY SIRONA. And it was the developments of August Maillefer’s company that became the “first signs” of modern endodontic instruments, without which effective, efficient and reliable treatment of periodontitis is impossible today.
Diagnosis of chronic apical periodontitis
Diagnosis of chronic apical periodontitis is similar to that in the case of acute apical periodontitis. This means we use basic and additional diagnostic methods.
The main ones include clarifying the patient’s complaints, medical history, probing, percussion, palpation and determining tooth mobility.
The patient’s complaints are most often absent, but they may complain of discomfort while eating when biting.
Probing is painless, palpation of the mucous membrane in the apical area is also painless. Percussion is weakly positive.
Additional special methods include determining the electrical excitability of the pulp (reduced to 200 μA), determining occlusion (the presence or absence of a traumatic factor), fistula tract, and temperature tests.
NB! We definitely do an X-ray examination.
How to prevent the development of the disease? Prevention
The main preventative point is the treatment of caries immediately after the onset of dental problems. The infection enters the periodontium through the carious area. To prevent marginal or marginal types of disease, in which the infection passes through the deep periodontal areas, it is important to monitor the condition of the gums. Periodontal treatment immediately after its appearance, as well as timely removal of tartar, is of great importance.
Acute forms of the disease are eliminated using an integrated approach to treatment in order to prevent the anomaly from moving to the chronic stage. This rule fully depends on the qualifications of the doctor and the availability of high-quality equipment in the clinic.