Dental sealants or dental sealants are a large group of synthetic plastics based on acrylic acid esters. The use of sealants as a means of caries prevention has become widespread. The method of using a sealant is to hermetically seal the fissures of chewing teeth.
Sealants are considered the only reliable method for the prevention of caries of the grooves of teeth, but the labor intensity of this method implies its infrequent use.
Fissure sealing - dental sealants
The main role in the origin of caries is played by soft plaque, consisting of polysaccharides, bacteria, and food debris. The length of time during which plaque remains on the tooth surface is directly proportional to the likelihood of developing caries. It is in order to remove accumulated plaque that dentists prescribe daily brushing of teeth. But some teeth, due to their structure, are more difficult to clean from plaque. Cleaning chewing teeth is labor-intensive primarily due to the narrowness and depth of the grooves covering their surface.
The bristles of a regular toothbrush are too large to penetrate the fissures to a depth that allows plaque removal. Due to the fact that the tooth enamel at the bottom of the fissure is thinner than on the rest of the surface, the process of carious lesions will develop faster and damage to the internal structures of the tooth will occur to a greater extent.
When filling the grooves of a tooth with dental sealant, its chewing surface will acquire a clearer contour and become smooth and flat. There will be no grooves on it that a toothbrush cannot penetrate. Removing plaque will become much easier, and the development of caries will be much less likely.
How does sealant work?
Oral hygiene in childhood is irregular and inadequate.
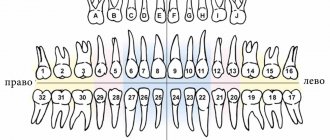
The chewing surface of molars and premolars is covered with anatomical grooves - fissures. Food particles remain in them, a layer of white plaque forms, which, without proper hygiene, leads to caries, then to pulpitis. For this reason, “sixes” (the first molars that appeared as a result of the change are located under this number) are treated or removed. Sealant is a liquid material consisting of acrylic-based synthetic plastic. When fissures are filled with sealant, the tooth surface becomes inaccessible to microbes. Food remains do not get stuck, and plaque removal becomes much easier.
Rationale for choosing a sealant for sealing fissures of permanent teeth in children
An urgent problem in pediatric dentistry is the prevention of fissure caries in permanent teeth, especially during the period of their eruption and mineralization in school-age children. Today there is no doubt about the need to use fissure sealing to prevent caries on the chewing surface of permanent teeth, however, in terms of the scale of preventive measures involving fissure sealing, our country lags behind many regions in which fissure sealing is an integral part of national successfully implemented caries prevention programs [3, 6 , 7, 9, 13].
INTRODUCTION
Fissure caries is one of the earliest and most common forms of destructive damage to hard dental tissues [2, 3, 6, 13]. Early damage to fissures is associated with the peculiarities of mineralization of tooth enamel: active maturation of tooth enamel occurs in the first 12–24 months, and in the fissure area continues for another 2–3 years compared to smooth tooth surfaces [6, 8, 9]. The high incidence of fissure caries is associated with the peculiarities of the anatomical structure of fissures, the accumulation of food debris and the formation of aggressive dental plaque in the natural recesses of the tooth [5, 14].
According to various authors, in children aged 7 to 12 years, the chewing surfaces of the first permanent molars are most often affected by caries [1, 10, 12, 13]. When they erupt, active growth of the jaws is observed, and a second physiological increase in the bite occurs. The destruction of these teeth by the carious process and untimely treatment leads to dentoalveolar deformities and the formation of various occlusion pathologies [4, 10, 11, 15].
Reducing the level of dental morbidity in children and adolescents, primarily dental caries, is a priority direction of modern dentistry. Children's age is the most promising for obtaining high rates of preventive measures.
Purpose of the study: to justify the choice of sealant for sealing fissures of permanent teeth in children to increase the effectiveness of caries prevention.
Research objectives
- To study the prevalence and intensity of caries of permanent teeth in children 7-8 and 12-13 years old living in Omsk.
- To assess the hygienic status of the oral cavity of schoolchildren using the Green-Vermillion index.
- To determine the level of awareness of practical healthcare doctors about fissure sealing.
- Justify the choice of material for fissure sealing.
Materials and research methods
To achieve this goal, we conducted an oral survey and questionnaire of parents whose children sought dental care. Parents and patients were informed about the examination methods and the purpose of the work being carried out, and voluntary informed consent to participate in the examination was obtained. The examination was carried out using a standard set of dental instruments. When conducting a clinical examination of children, we used the Riga map. The Riga map is convenient and informative for such studies and includes the following indices: KPU+kp, kp, KPU surfaces and KPU cavities. The hygienic state of the oral cavity in children was determined using the Green-Vermillion hygiene index (1964), which allows one to assess the presence of not only plaque, but also tartar.
The electrical conductivity of hard dental tissues was measured using the Dentest device. To assess the thixotropy of the sealants, microphotography of teeth sections was carried out using an electron microscope.
Results
To solve these problems, we examined 64 children of Omsk aged 7-8 and 12-13 years, students of secondary schools No. 28 and 83. 38 girls were examined, 26 boys.
During a dental examination of schoolchildren aged 7-8 and 12-13 years, it was revealed that the prevalence of caries in permanent teeth is quite high and reaches 86%. The intensity of caries in permanent teeth (CPD) also increases with age and is: at 7-8 years old - 3.8, at 12-13 years old - 4.3. A structural analysis of the KPU indicators revealed that the growth of the KPU index is mainly due to the growth of the “K” indicators. In children aged 7-8 years it is 59%, in 12-13-year-old peers it increases to 69%. With age, there is a tendency for the “P” indicator to increase: for 7-8 year olds it is 41%, for 12-13 year olds it is 29%. However, in all age groups, the “K” component significantly exceeds the “P” component, which indicates untimely receipt of dental care. In the structure of the index of permanent teeth, there is an almost complete absence of “U” indicators in all age groups: only in 12-13 year olds it was 2% (Fig. 1).
Rice. 1. Assessment of indicators K, P, U depending on age.
At the same time, there is also a predominant lesion of the chewing surfaces (at 7-8 years old - 39%, at 12-13 years old - 46%) compared to the vestibular surface (at 7-8 years old - 18%, at 12-13 years old - 19%) , medial contact (in 7-8 years - 16%, in 12-13 years -11%), distal contact (in 7-8 years - 22%, in 12-13 years -17%) and oral (in 7-8 years old - 5%, 12-13 years old - 7%) (Fig. 2).
Rice. 2. Prevalence of caries on various surfaces of permanent teeth in children.
Using the Dentest device, the degree of mineralization of the enamel of permanent teeth (4.6 and 1.1) was determined in children 7-8 years old. The initial level of mineralization (ILM) of the 4.6 tooth enamel on the buccal surface averaged 7.4±0.8 (high ILM), and on the chewing surface - 22.5±1.5 (average ILM). For comparison, the IUM of 1.1 teeth was measured in the area of the cutting edge - 0.3±0.2 (high IUM), and in the cervical area - 6.4±0.7 (high IUM). Our results confirm the opinion of a number of authors [6, 8, 9] that the maturation of enamel on a smooth surface has a higher rate of mineralization compared to occlusal surfaces. In this regard, the occurrence of caries on the chewing surface can be predicted with a 50% probability [9]. High rates of caries damage to chewing surfaces and a low initial level of mineralization indicate the need to prevent caries in permanent teeth in children.
A fairly high intensity of caries damage to the chewing surfaces of permanent teeth was revealed against the background of unsatisfactory oral hygiene in the age groups studied. The value of the initial hygiene index in children 7-8 years old reached 2.7, in children 12-13 years old - 2.6. Thus, the high incidence of caries on the chewing surfaces of permanent teeth, combined with a low level of oral hygiene, confirms the need for schoolchildren to carry out preventive measures to prevent caries of chewing surfaces using the fissure sealing method.
To improve the hygienic state of the oral cavity, health lessons were conducted for schoolchildren, which included teaching schoolchildren how to brush their teeth with a demonstration of brushing teeth on models (Fig. 3) and dental education for 5 lessons.
Rice. 3. Teaching children oral hygiene.
The result revealed a significant improvement in the level of oral hygiene after 5 lessons; the index value decreased significantly in all age groups. In the first age group (7-8 years), the index decreased by 1.5 (56%) and amounted to 1.2. In the second age group (12-13 years), we observed a similar picture, the index decreased by 1.7 (66%) and amounted to 0.9.
To study the level of awareness of pediatric dentists about fissure sealing, we conducted a survey of 70 pediatric dentists in 4 public and 8 private clinics in Omsk. The doctors' work experience averaged 20±5 years. The following results were obtained during the study: 82% of doctors consider the use of sealants to be effective for the prevention of caries, 86% of dentists, using fissure sealing in their practice, stated that there was no caries damage to chewing surfaces.
However, only 27% of doctors use sealants in their practice quite often, 63% rarely, and 10% do not use them at all (Fig. 4).
Rice. 4. Application of fissure sealing at a dental appointment.
There are a large number of different materials for sealing dental fissures; it is difficult for practicing dentists to navigate when choosing the most effective caries preventative agent. The most commonly used sealants are: Fissurit F, Fissurit FX, Ionosit Seal, Delton, Fissil - S, Fissulight LC (Fig. 5).
Rice. 5. Demand for materials for fissure sealing by dentists.
As the survey showed, the most commonly used sealant is Fissurit F, and the least used is Fissulight LC. To study the reason for this choice, it was decided to study one of the most important properties of sealants—thixotropy. To study the thixotropy of sealants, fissure sealing was carried out on extracted teeth. We studied 12 healthy teeth removed for orthodontic reasons. The extracted teeth were divided into 2 groups (6 teeth in each) depending on the sealant used. Sealants Fissurit F, “Fissulight LC” - light curing. After sealing, the tooth was sawed longitudinally and examined under an electron microscope. Photographs were taken from the samples obtained. The results of our electron microscopic study of the sealants Fissurit F (Fig. 6), “Fissulight LC” (Fig. 7) revealed that Fissurit F has the best thixotropy.
Rice. 6. Fissure sealing “Fissulight LC”. Rice. 7. Fissure sealing “Fissulight LC”.
The ability of the sealant to penetrate even into closed fissures provides a high caries-preventive effect, which explains the choice of Fissurit F by most of the doctors surveyed and gives grounds for recommending this sealant for sealing fissures.
Analyzing the results obtained, we can draw the following conclusions:
- the prevalence and intensity of caries of permanent teeth in children 7-8 and 12-13 years old in Omsk is high;
- the state of oral hygiene of schoolchildren according to the Green-Vermillion index is unsatisfactory;
- despite the high level of awareness of practical healthcare doctors about fissure sealing, this area of prevention is used in practice quite rarely;
- the choice of sealant for sealing fissures plays an important role in the effectiveness of the prevention; The most preferred sealant is Fissurit F.
LITERATURE
- Alimsky A.V., Fleisher G.L. Modern prerequisites and real opportunities for organizing hygienic training and dental education among the children's population of Russia. Medical alphabet // Dentistry. - III/2010.
- Boyarkina E. S. Development and evaluation of the effectiveness of minimally invasive methods for the treatment of fissure caries of permanent teeth in children (clinical and laboratory study): abstract. dis. ...cand. medical sciences - M., 2009. - 19 p.
- Bryanskaya M.N. Clinical and morphological rationale for the prevention and treatment of fissure caries of permanent teeth with immature enamel: abstract. dis...cand. honey. Sci. - Irkutsk, 2009. - 23 p.
- Vagner V. D., Distel V. A., Karnitsky A. V., Mateshuk A. I., Suntsov V. G. Guide to practical training in orthodontics. - Omsk: Publishing House Omsk State Medical Academy, 2009. - 372 p.
- Vlasova G. I., Lugovskov D. A., Silaeva O. A., Dudar S. V. Clinical assessment of the prognostic significance of informative markers in the practice of preventive dentistry // Ukrainian Medical Almanac. - 2008. - Volume 11, No. 5. - P.37-38.
- Zhorova T.N. The process of enamel maturation after eruption and the influence of various factors on it: Dis. Candidate of Medical Sciences Sci. - Omsk, 1989. - 24 p.; Leontyev V.K. Caries and mineralization processes: Abstract of thesis. dis. - Omsk, 1978. — 45 s.
- Kutsevlyak V.F., Polyakova S.V., Pushkar L.Yu., Varakuta V.V., Grishchenko V.V., Volkov S.N. Fissure sealing is a method of modern caries prevention.
- Leontyev V.K. Caries and mineralization processes: Abstract of thesis. dis. - Omsk, 1978. - 45 p.
Types of materials
Types of sealants:
- chemical and light-curing
- transparent and colored.
Materials with a colorless texture are used if the dentist suspects the likelihood of rapid development of caries. In this case, the surface of the tooth is observed. The appearance of caries is visible through the sealant. If there is no suspicion, the surface is coated with colored sealants so that their abrasion is immediately noticeable to parents. If there is no longer any colored sealant on the tooth, it’s time to go to the dentist to seal the fissures.
What are dental sealants?
Dental sealants are a type of bioplastic that is poured into fissures in liquid form to seal them. The use of plastic is explained by the fact that the material does not damage the enamel and does not cause an allergic or oxidative reaction.
The purpose of their use is the prevention of caries. The material can be transparent or colored, which attracts children. The sealant is used primarily for permanent chewing teeth with deep fissures. Sealing baby teeth is considered impractical, since caries of primary teeth develops quickly and cannot be stopped using this method.
The sealant has the property of being evenly distributed over the surface, neatly filling all the grooves. After the plastic hardens, its surface becomes even and smooth.
At what age are sealants used?
The surface of the tooth is sealed at 5-7 and 12-14 years. Only permanent teeth are covered with sealant. At an early age, oral hygiene skills are not sufficiently developed, and the procedure protects against the proliferation of pathogenic microflora on the surface and in the recesses of the teeth. The coverage condition is a completely healthy tooth without fillings or caries installed on it. Remember, even while a tooth is erupting, it is susceptible to caries. Therefore, as soon as the chewing surface of a permanent tooth has erupted, consult your dentist about fissure sealing. Sealing is also prescribed for adults, but a recommendation on the appropriateness of the coating is obtained from the dentist.
Contraindications
There are a number of contraindications, in the presence of which the installation of dental sealants is difficult or impossible. This is a long period of eruption; lack of satisfactory oral hygiene; the presence of a carious cavity in the tooth; caries in the form of decompensation.
About the advantages. Properly installed sealants last up to five years. The sealant is guaranteed to protect tooth enamel from carious damage for a specified period.
If the sealant falls out of the tooth or damages the integrity of the dental sealant, you must immediately contact your dentist.
Installation and reinstallation of sealant is possible and should be done after consultation with your dentist. Moscow metro station Zvezdnaya, Danube Avenue, 23
Fissure sealing procedure
1. Professional teeth cleaning. The dentist uses brushes to remove plaque.
2. Rinse the treated teeth with distilled water, isolate from saliva with cotton swabs.
3. Coating with a special compound that makes the surface rough and improves the adhesion of the sealant to the fissure.
4. Rinse and dry teeth, treat with sealant, remove excess material.
5. Checking the filling of fissures using a polymerization lamp. The same device acts on the sealant, as a result of which the composition hardens.
6. Check for absence of interference when closing the jaws.
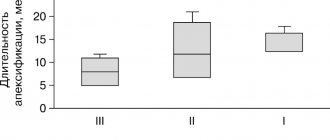
7. Removing excess hardened sealant with diamond or carborundum nozzles.
8. Duration of reception - 15-60 minutes. The amount of time depends on the amount of work the dentist does. Fissure sealing is painless and children tolerate it easily.
Service life of sealants
Guarantee of tooth protection and prevention of caries using sealant coating - from 3 to 5 years. If the sealant is damaged or falls out of the fissure, you need to see a dentist and repeat the procedure.
Differences between sealant and filling
1. Coating with sealants does not require drilling the tooth.
2. The content of fluoride ions in the composition strengthens the enamel, unlike fillings.
3. The age of installation of sealants is up to 25 years.
On the issue of fissure sealing
Today, dentists around the world unanimously recommend fissure sealing as the most effective method of caries prevention in both temporary and permanent teeth.
Sealing fissures and natural cavities with sealants is a very effective measure for preventing caries in these areas. The widespread use of sealants (sealants) has significantly reduced the incidence of dental caries, along with the use of fluoride and other preventative treatments.
The use of modern materials (sealants) for fissure sealing has undeniable advantages. They prevent plaque from getting stuck in the recesses, plus they release fluoride ions for a long time; the preventive effect is maintained even after a visible reduction in the amount of material, since the sealant particles still remain deep in the fissures.
What you need to know about the fissure sealing procedure:
- the procedure is absolutely painless and does not require local anesthesia;
- A distinction is made between invasive and non-invasive fissure sealing. When carrying out an invasive fissure sealing technique, fissure grinding is additionally carried out;
- Fissure sealing of one tooth takes about 5 minutes;
- fissure sealing is carried out on both permanent and temporary (baby) teeth;
- sealing technique:
- cleaning teeth from plaque using a special brush and paste,
- isolation of the tooth from saliva,
- treatment with a special composition to create a mechanical bond between the sealant and tooth enamel,
- rinsing and drying the tooth,
- applying a sealant (sealant),
- polymerization of the material,
- occlusion check.
Thus, you can quickly and painlessly protect your tooth from caries for 1.5-2 years; it is important to realize that a sealed tooth requires monitoring. Periodic observations and replacement of the sealant (if necessary), along with the use of fluoro- and calcium-containing preparations that strengthen the enamel, will ensure almost 100% absence of caries.
Seal now or drill later - the choice is yours, dear parents! We hope you make the right choice.
You can make an appointment or ask any questions from our administrator by calling +7(929)576-02-04.
Why are sealants used in dentistry?
The chewing group of teeth, or premolars and molars (4th–8th teeth), are most suitable for chewing, that is, grinding and grinding food. This function is due to their structure - the surface between the chewing cusps of the tooth is covered with numerous grooves, depressions and grooves, which are called fissures. Dental plaque accumulates in these natural “folds” of enamel, which is quite difficult to remove when brushing. caries often develops here .
It is known that fissure caries is one of the earliest and most common forms of the disease. According to some studies, by the age of 18 in dental clinic patients, the chewing surface of most molars is affected by caries or filled [1].
In order to protect teeth from fissure caries, among other methods, the procedure of sealing, or sealing, fissures using dental dental sealants is used. These are special materials based on composites, which contain fluorine and calcium, which remineralize and strengthen the enamel.
The preventive effect of sealants is ensured by performing two important functions:
- creating a durable coating on the enamel surface that prevents the effects of factors that cause caries;
- participation in the mineralization of enamel if the sealant contains fluorides.
Sealing technique
Obturation can be performed using a non-invasive (simple) method or an invasive one. When non-invasively sealing the fissures of permanent teeth, the first step is to clean the chewing surface and dry the tooth. The area between the tubercles is treated with a substance that increases the adhesion of the sealant to the enamel, then the recesses are sealed with the material.
The invasive method involves changing the shape of the fissure grooves and removing discolored (demineralized) areas. To do this, after examination and thorough cleaning, the fissures are opened: using a bur, a small layer of enamel is removed to remove areas where food usually gets stuck. After opening, the surface of the tooth can be better examined for caries that have already begun. If there are no lesions, the recesses are obturated with the selected sealant.
When choosing a technique, a specialist during examination and diagnosis must evaluate the type of structure and depth of the grooves, the prevalence of caries when detected, as well as the properties of the enamel. There are the following types of fissures, differing in anatomical structure, which can be very complex in some patients, and the degree of mineralization:
- funnel-shaped;
- cone-shaped;
- teardrop-shaped;
- polyp-like.
Funnel-shaped fissures have the most favorable anatomical shape - they are well mineralized, open, and in the absence of signs of demineralization (discoloration, rough surface) may not require filling with a sealant. With other types, food debris may get stuck and not washed out with saliva or during cleaning for a long time, which creates conditions for the proliferation of cariogenic bacteria. In such cases, invasive fissure sealing is often used as a preventative measure against the development of caries.
How long do sealants last?
There are different types of dental sealants. They may differ in basic characteristics, properties and cost. Most types of sealants add minerals to strengthen the weak enamel of molars.
Caries prevention by fissure sealing is carried out to preserve permanent teeth, so many parents are concerned about how long sealants can last, because it can take a long time for fissures to fully form.
Conducted studies confirm that if you follow the dentist’s recommendations and properly care for your oral cavity, the service life of the sealant can be at least 5 years. Thus, the child’s teeth will be protected from caries and most of its complications until the dental system is fully formed. Regular preventive examinations will allow timely detection of violations in the tightness of fissures and carry out the necessary manipulations to eliminate them.
The use of dental sealants in pediatric dentistry is the right decision. After all, by keeping your permanent teeth healthy, you can avoid not only complex treatment, but also many other pathologies that caries of permanent molars leads to.
What are sealants
Dental sealants are special composite resins, or sealants, typically cured with light or chemicals. Several classes of materials are used as dental sealants, in particular:
- composite chemo- and photocurable materials;
- glass ionomer cements;
- compomers.
Sealants have high fluidity, thanks to which they easily fill even thin and narrow fissures to the very bottom. Thanks to this, the chewing surface of the teeth is leveled, and their hygiene becomes easier.
There are filled and unfilled sealants. Unfilled sealants are more fluid, but less durable and wear out faster. Filled - have a smaller penetration depth, but are more durable and less susceptible to abrasion. Filled sealants are used for invasive sealing procedures.
The applied dental sealant is permeable to mineral substances contained in the oral fluid, and therefore does not interfere with the mineralization of the enamel. Metabolic processes under the coating in the hard tissues of the tooth are maintained at a physiological level. In addition, many sealants are specially enriched with fluoride and calcium, which strengthen the enamel. At the same time, large molecules, such as proteins, are not allowed to pass through the sealant layer.
Sealing with glass ionomer cements
Glass ionomer cement is used in various branches of dentistry: as a crown-fixing material, for permanent fillings in children and temporary fillings in adults. The use of GIC as a sealant is widespread due to its physical properties and chemical properties. The main advantage of the material is the ability to saturate the enamel with fluoride ions.
In adults, GIC can be used to seal fissures when:
- thin enamel, signs of hypersensitivity;
- detection of areas of demineralization;
- inability to completely dry the surface;
- low caries resistance.
Tooth enamel is built from many hydroxyapatite crystals, packed in a special way for high strength. One of the most unfavorable cariogenic factors affecting the enamel layer is organic acids formed during the activity of bacteria. Fluoride, embedded in the shell of hydroxyapatite, significantly increases the resistance of hard tissues to dissolution by acids, and thus protects teeth from caries. Glass ionomer cement sealant releases fluoride most actively in the first hours after application. During the rest of the time it remains a reservoir of ions. Fluoride from the sealant is released not only directly into the place of contact with the enamel, but also into the surrounding saliva, which constantly ensures the content of beneficial ions in the entire oral cavity and additional prevention against caries of other teeth.
Both light-curing and chemical-curing GIC can be used as a filler. The first type of sealant is more expensive, but it is more convenient to use, which improves the quality of the sealing produced, and its complete hardening occurs in a few seconds under the light of a dental photopolymerizing lamp. Chemically cured cements take several hours to fully cure after application. This requires compliance with additional rules after the procedure (gentle brushing of teeth, avoidance of solid foods at first).