Most dental patients want to have not just a healthy, but also an attractive smile. Unfortunately, not everyone can boast of this.
Back in 1984, some components that are necessarily inherent in a “beautiful smile” were identified:
- The smile should expose almost 100% of the coronal part of the tooth and the gingival papillae, while the gum itself should not be visible (otherwise, when the gum is exposed, we are talking about a “gummy smile”).
- The gingival contour should be symmetrical, smooth, the edges of the gums at the central incisors and canines should be located at the same level, and at the second incisors - 1-2 mm lower.
- The length of the tooth crown should not be less than 11 mm, and the width should correspond to the “golden ratio”.
- The gum contour should be in harmony with the smile line.
If the patient's smile does not fit into these standards, then it can be significantly improved by changing the edge of the gingival contour and increasing the length of the dental crown.
Contraindications
Lengthening is not suitable in some cases, so dentists do not recommend surgery in the presence of the following conditions:
- the tooth has a short root;
- the biological width of the dental element is not enough;
- in cases where the expended efforts and resources are not justified and it is easier to carry out prosthetics;
- there is not enough space between the tooth and the antagonist;
- if the appearance of the tooth or adjacent elements deteriorates.
Professional dentists determine the feasibility in each case individually.
Contraindications to lengthening the clinical crown of a tooth
In some cases, after weighing all the pros and cons, the dentist may refuse to lengthen the patient’s dental crowns.
The following reasons may serve as the basis for this:
- After tooth crown lengthening, the appearance and health of adjacent teeth will deteriorate.
- Regardless of the lengthening, restoration of this tooth is still impossible.
- Insufficient biological width.
- A tooth with a short crown has a short root.
- During orthodontic lengthening, there is no space between the tooth that is planned to be lengthened and the opposing tooth.
- The ratio of the effort required to lengthen the crown of a tooth and its value is not in favor of preserving the tooth.
- The patient is unable to maintain the required level of periodontal health.
Removal methods
Dentists offer four ways to lengthen the crown:
1. Surgical. During surgery, part of the gum and/or bone is removed. It is carried out in the form of gingivoplasty, gingivectomy and bone resection.
2. Therapeutic. Composite extension in the incisal area. It is effective for small chips and chips.
3. Orthodontic. The tooth is stretched using braces. The method is allowed if there is free space between the teeth and is recommended when lengthening one tooth that differs in length from the rest.
4. Orthopedic. Extension is performed using veneers or crowns. The tooth is lengthened due to the crown part without changing the gingival zone.
In what cases is it necessary to lengthen the clinical crown of a tooth?
Lengthening the clinical crown of a tooth may be prescribed to a patient for the following reasons:
- Aesthetic
- "Gummy" smile.
- Violation of the gum contour of one or more teeth.
- The natural crowns of the teeth are too short - after eruption the gums did not rise and remained “lowered” on the tooth.
- Under-eruption of one or more teeth in the dentition.
- To improve dental hygiene.
- Tooth-preserving
- The need to restore the length of teeth that was lost as a result of pathological abrasion (bruxism, increased tone of the masticatory muscles can lead to this).
- The presence of caries in the subgingival part of the tooth, i.e. below the gum line.
- The need to carry out and maintain high-quality tooth restoration using any of the methods, because to maintain periodontal health, such restoration should not go below the gum level.
- For high-quality prosthetics, in case of complete destruction of the tooth crown, for reliable “full” capture of the hard tissues of the tooth and to prevent future problems with the crown.
- As one of the components of complex surgical treatment of periodontal diseases for the removal of periodontal pockets.
What should you pay attention to?
The procedure must be performed flawlessly, as even a minor mistake can cause cosmetic defects and loss of tooth stability. It is important to conduct thorough preparation, including extensive diagnostics. It includes a computed tomography scan, consultations with an orthopedist, surgeon and periodontist. This will allow you to correctly assess the condition of the jaw tissue and determine the length of the roots.
When preparing for lengthening, all points are taken into account:
- bone condition;
- aesthetics;
- condition of periodontal tissues;
- the distance between the bone crest and the gingival sulcus (should not be more than 3 mm);
- anatomy of dental roots and their relationship to the coronal part.
What does a patient need to know about lengthening the clinical crown of a tooth?
In order for the tooth crown lengthening procedure to be successful, it must be carefully and comprehensively planned - this applies to all methods of its implementation. In planning such treatment, depending on the chosen intervention technique, several specialists will take part - a periodontist, a dental surgeon and/or an orthodontist, a dental therapist and/or an orthopedic dentist.
When planning to determine the volume and type of intervention, the following are taken into account:
- Current and future health status of periodontal tissues.
- The proportions of the tooth itself, the aesthetics of the patient’s smile.
- The structure of the roots of the tooth and the ratio of the length of the root and crown. It is IMPORTANT that its root part is no less visible.
- Condition of the jaw bone.
- Biological width is the distance from the bottom of the gingival sulcus to the crest of the tooth-bearing bone, and in order for the tooth to be stable in the future, its value must be at least 3 mm.
Therefore, lengthening the clinical crown of a tooth requires a very careful diagnosis, because the procedure should not disrupt the stability of the teeth on which it will be performed.
Diagnostics before tooth crown lengthening includes:
- Assessment of periodontal condition (diagnosis by a periodontist).
- Diagnosis by a surgeon – if a surgical lengthening method is proposed.
- Consultation and diagnosis with an orthopedist – in case of need for extensive restorations, prosthetics or the use of an orthopedic lengthening method.
- Consultation with an orthodontist and orthodontic diagnosis, if the crown will be lengthened by installing a brace system
One of the mandatory studies during diagnosis will be a 3D CT scan - computed tomogram, to determine the length, location of the tooth root and the condition of the jaw bone tissue.
Operation stages
Most often, hygivoplasty is performed, which involves excision of the gum along the gingival contour. In some cases, part of the bone may be removed.
The operation is performed in a surgical room under local anesthesia or general anesthesia (in some cases). Preliminary sanitation is required.
The procedure itself takes place with the following steps:
- if bone resection is necessary, the flap is peeled off and an osteotomy is performed;
- a new contour is formed, which is located higher;
- stitches and a gum bandage are applied to the wound;
- For healing and recovery, antiseptic rinses are prescribed; in some cases, antibiotics are recommended. Chewing and physical activity are limited;
- removal of sutures - after 7-10 days;
- after healing, prosthetics or restoration are carried out (if temporary structures are installed, they are replaced with permanent ones after complete healing).
Final recovery occurs after 1-3 years.
The perfect smile of Hollywood stars
Dental services in America are noticeably expensive. For this reason, more aesthetic and image prosthetics are carried out there, and medical procedures often remain in the shadows. The new teeth of famous personalities are often displayed like an expensive car. Unfortunately, the Hollywood smile is not for everyone. Perhaps you have noticed how comical teeth sometimes look in some photos.
The effect of “artificial dentures” is not at all what modern aesthetic dentistry strives for. Your smile should be natural and healthy, highlighting your individuality. A harmonious, attractive smile, what is it like according to the majority of our compatriots?
Cost of services
Surgery Price
Lengthening the crown of a tooth from 1000 rubles.
Expert of the article you are reading:
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
You may also be interested in:
Wisdom tooth removal Tooth extraction Removal of the dental nerve Complex tooth extraction Resection of the apex of the tooth root Removal of an impacted tooth Removal of the tooth root Removal of a dystopic tooth
Show more
We create a unique, beautiful smile
A beautiful smile is not a privilege, but a requirement of our dynamic times, as well as a significant part of the image of every business person. But what makes a smile unique? First of all, it is the harmony of color, size, shape and position of the teeth. In addition, your teeth should have an optimal relationship with your facial structures.
Today, a technology has been developed for calculating the correct height of the tooth crown. It combines a mathematical calculation and a biological component, in this case the color of the iris.
Taking into account the biological characteristics of each person, beauty salon specialists will form a smile that will give the patient maximum self-confidence.
Surgical Crown Lengthening for Distal Restorations
Today, more and more often, in distal restorations, we are seeing the technique of raising the deep subgingival margin (Deep Margin Elevation). It is performed in clinical situations where it will be necessary to perform bone correction surgery and surgical crown lengthening. We emphasize that the procedure for raising the deep subgingival margin, recently introduced by Professor Pascal Magne, Dr. Didier Dietsky and Dr. Roberto Sprafico, is used in borderline clinical situations where rubber dam isolation is difficult but still possible; in cases where it is necessary to facilitate impression taking and subsequent isolation for bonding, and, importantly, in those clinical situations where the biological width of the periodontium is still present.
Author: Giuseppe Marchetti
The concept of biological width, postulated by Gargiulo et al in 1961, is a fundamental requirement when performing restorations and prosthetics. The biological width must be observed both when performing restorations and prosthetics, otherwise there is a high risk of creating iatrogenic periodontal pockets.
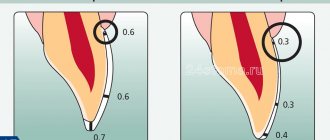
In this article we want to demonstrate the technique using simple and easily repeatable illustrations without performing DMA. The procedure consists of the following steps. First, the carious cavity is prepared to prepare the cervical edge, which should no longer move apically. Then - an operation to place the bone crest 3 mm below the already prepared cervical edge. And finally, the restoration itself. Carrying out surgery before preparing the cervical edge is a big mistake, because... often results in the need to perform DMA.
Photo 1 – Bitewing before treatment. Large carious cavity on the distal surface 1.6.
Photo 2 – In the oral cavity.
Photo 3 – After preparation, the need for surgical lengthening of the crown becomes obvious.
Photo 4 – Preparation of the carious cavity, distal cervical edge and surgical lengthening.
Photo 5 – It is necessary that the bone crest is 3 mm below the cervical part of the tooth crown.
Photo 6 – Suturing.
Photo 7 – Insulation using rubber dam. Note the good isolation obtained from the surgical procedure.
Figure 8 – The thickness of the palatal and distal cusps was less than 2 mm, so they were removed. In fact, we removed all bumps thinner than 2 mm. Advice: when preparing for a composite onlay inlay, the height must be reduced by 2 mm, for a lithium disilicate inlay - by 1 mm.
Photo 9 – Build-up, sealing of dentinal tubules, preparation for onlay inlay was carried out. Advice. Clean the dentin with glycine powder and disinfect it with chlorhexidine 2%. Then etch the enamel for 20 seconds and apply a universal self-etch adhesive to the dentin and enamel. This will allow you to avoid post-operative soreness.
Photo 10 - Only at this stage can we prepare and restore with direct restorations 1.5 and 1.7. Advice: do not do this earlier so as not to damage the restoration during the preparation of tooth 1.6 under onlay.
Photo 11 – Installation of sectional matrices and wooden wedges.
Photo 12 – Direct restorations on 1.5 and 1.7 are made in A2 shade, with brown stain added to increase the perception of depth. Finishing and polishing has been carried out. Tip 1: Use a universal self-etching bond using the selective etch technique. This will ensure the best result without any post-operative sensitivity. Tip 2: For perfect control of the working field and the absence of blood or saliva in it, finishing of restorations should be carried out in a rubber dam.
Photo 13 – Occlusal contacts are checked before impressions are taken and no corrections are required. Tip: Be sure to check the occlusal relationship and make corrections if necessary before taking impressions.
Photo 14 – Imprint. Advice: to get a result with the least distortion, it is better to make a one-stage, two-phase impression.
Photo 15 – Composite onlay tab on the model.
Photo 16 – After 48 hours, the insert is fitted without a rubber dam. The stitches are still not removed.
Photo 17 – Checking occlusion.
Photo 18 – Setting up the rubber dam, fitting the inlay already in the rubber dam WITHOUT bonding.
Photo 19 – Fixing, finishing and polishing.
Photo 20 - Checking the occlusion after fixing the inlay demonstrates that there is no need for correction.
Photo 21 – Final inspection of three restorations.
Photo 22 – Two weeks after surgery, good integration of restorations 1.5 1.6 1.7.
Photo 23 – Details of morphology and anatomy 1.5 1.6 1.7.
Photo 24 - Details of restorations. The tissues heal, but full recovery will occur in six months.
Photo 25 - Final X-ray. Good accuracy of the restorations was shown.
conclusions
To restore means to restore the function and aesthetics of our patients’ teeth. The restoration must be done accurately and accurately, and also last a long time. To get good results, we must follow simple rules and protocols without any flights of fancy.
If these rules are feasible, predictable and applicable, we will achieve the results we require.
After all, universal adhesives are now showing excellent results. This is not the future of adhesion, but the present, so use them without fear or doubt.
The author wishes to thank Dr. Paolo Marchetti for surgical procedures and Mr. Sebastiano Nardo for laboratory work.
The translation was performed by T. Skovorodko specifically for the OHI-S.COM website. Please, when copying material, do not forget to provide a link to the current page.
https://www.styleitaliano.org/
When should you see a doctor?
Dentist help is necessary if one of the incisors is in a high or low position. In children, this defect can disappear without any intervention when replacing milk teeth with molars. If different lengths of the front teeth persist despite a fully formed bite, you should consult a doctor.
You should also contact a specialist:
- when the enamel darkens,
- increased sensitivity of teeth,
- acute toothache,
- cutter mobility,
- formation of a sharp cutting edge.
The dentist will conduct an examination, determine the cause of the problem and help solve the problem.
Preparation for the procedure
For the procedure to be successful, an examination must be carried out before it begins. It includes an assessment of the structure and condition of the tooth roots, their relationship with the crown, the condition of the jaw bones and gum tissue. The patient’s oral cavity is also examined for carious lesions and inflammatory processes in the oral cavity.
For more effective diagnosis and treatment, an additional consultation with an orthopedic dentist, periodontist or surgeon may be required. A CT scan is also performed to see the length and location of the roots hidden under the gum tissue. The last stage of preparation is professional teeth cleaning and antiseptic treatment of the oral cavity.
What could be the consequences?
The problem most often manifests itself exclusively from an aesthetic point of view - psychological problems arise, the patient wants to correct the pathology as quickly as possible, especially if it is pronounced. That is, if the teeth and gums are healthy, then such discomfort is the only consequence of the problem.
If the short size of the crowns is caused by an abnormal structure of the teeth, problems with the gums, or abrasion of the enamel, then the consequence of this condition may be inadequate chewing of food, which will inevitably lead to problems with the gastrointestinal tract, premature aging of the face and the appearance of deep wrinkles near the mouth, and general deterioration dental conditions and even their loss.
The need for surgery
An operation to lengthen the crown of a tooth is prescribed to a patient for several reasons:
Aesthetic reasons:
- the gum frame is damaged;
- discrepancy between the height of the gum and teeth;
- improving dental hygiene;
- not fully erupted teeth.
Preservation of teeth:
- the need to restore the length of a dental unit lost as a result of abrasion;
- the presence of caries under the gums;
- the need for dental restoration work.
Periodontal causes:
- effective periodontal treatment.
Causes
causes of row lengthening are:
- pathological change in respiratory function with oral predominance;
- disruption of the swallowing process with the formation of the infantile type;
- pronounced articulation of the tongue during conversation;
- the presence of bad habits with the manifestation of obsessive movements: sucking a finger, pacifier or tongue, chewing a pencil and other objects;
- macrodentia, with the formation of several abnormal teeth;
- remote or abnormal position of the buds, with the growth of which a trema or diastema is formed between the teeth.
Several anatomical factors can be identified, for example, the eruption of supernumerary teeth during the primary dentition period or the failure of teeth to fall out during a change in occlusion.
Diagnostics
When visiting a dentist, a patient expects comprehensive care, healthy teeth and comfortable dentures, but, unfortunately, not all dentists can do this. A small dental office, where a private doctor works, does not have complex diagnostic equipment (for example, an orthopantomograph or a computed tomograph), and does not use a microscope, since this is also too expensive for a private doctor. Another problem of small clinics or private offices is that when situations arise when surgical intervention or complex treatment of tooth canals is required with retreatment, extraction of fragments, etc., the doctor suggests removing the tooth as hopeless, since he can cope with it on his own. problem, and doesn’t want to lose the patient by sending him to another clinic. It would seem that what problems - the tooth was removed and an implant or bridge was installed - the problem was solved. But if there is hope of saving your own tooth, even the root of it, it is better to turn to an experienced doctor who will save the tooth.
At Family Dentistry, when a question arises whether to treat a tooth or remove it, a decision is made only after a comprehensive examination and analysis of the situation. This is possible thanks to the availability of modern X-ray diagnostic equipment in the clinic, including a computed tomograph, and the well-coordinated work of specialists - endodontists working with microscopes, surgeons, prosthetists, dental technicians - who are able to find a joint solution in the most difficult cases.
This work reflects only one part of the complex treatment that was performed by Dial-Dent specialists to put all of this patient’s teeth in order. There were a lot of problems, but the peculiarity of Family Dentistry is precisely the solution of complex cases that require complex treatment. In the near future, other stages of treatment will be described: dental implantation and prosthetics on implants, aesthetic prosthetics, dental restoration, caries treatment.
For general diagnostics, a panoramic photograph of the teeth was taken. In a fragment of a panoramic image, arrows show the teeth considered in this work at the top left. Existing problems:
- Voids inside previously treated canals - which indicates unsatisfactory quality of treatment.
- An overhanging edge of the crown that catches food.
- A pin in a tooth made of unknown material.
- Crowns combined into one design.
The appearance of old crowns is unsatisfactory (the teeth in question are shown with arrows). Upon examination, it is clear that the edge of the crown hangs over the gum, food gets stuffed under it, which leads to injury and inflammation of the gums, the crowns are made in the form of a combined structure, which is extremely unfavorable for the roots of the teeth, as they become loose, as well as for the interdental papilla of the gums - the combined structure led to its inflammation:
It was decided to redo the crowns, so the old crowns were removed. Under the crowns there was severe inflammation of the gums (1), one tooth was reinforced with a metal pin (2), the teeth had caries, and one of the teeth had an old filling that went under the gum, which complicates treatment (3).
View of teeth from the inside:
External view of teeth:
How is the rehabilitation going?
In order to avoid complications and recover as quickly as possible, the patient must strictly follow the recommendations of the attending physician. He needs to rinse with an antiseptic and take antibiotics and pharmacological painkillers. In the first days, you need to minimize physical and chewing stress.
The sutures are removed after about a week. After the wound has healed, temporary prosthetics or restoration are performed, which are replaced with a permanent one after a few months. Complete restoration of the gum edge occurs in one to three years.
Preventive recommendations
After surgery, the rehabilitation period is at least two weeks. During this time, the specialist prescribes the patient to take painkillers and mouth rinses. During the rehabilitation period, it is necessary to minimize the load on the gums, avoid eating solid foods and foods that require thorough chewing, carefully brush your teeth, and stop smoking and drinking alcoholic beverages.
When installing braces, you must follow the rules of oral hygiene so that food particles do not accumulate between the elements of their design and do not provoke infection of the gum tissue or the proliferation of harmful microorganisms. When choosing this method, you need to regularly visit the doctor on the appointed dates so that he can regulate the braces and monitor the rehabilitation process.