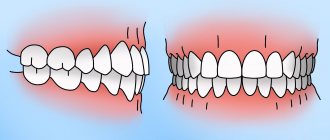
Abnormal bite is a common occurrence. With this pathology, there is usually a decrease or increase in the size of one jaw relative to the other, shifts forward or backward, reversals, deviations and displacements to the sides. Teeth do not fit together correctly, become crowded, or have gaps between them. Osteotomy in dentistry - artificial excision of the problematic jaw bone to correct the bite - is a radical and relatively traumatic, but effective approach to eliminating such anomalies.
Consequences of a broken bite
If you leave the problem for many years and do not resort to surgical intervention, there is a high risk of encountering serious orthodontic, gastroenterological and other problems:
- inability to chew food thoroughly, leading to gastrointestinal diseases;
- uneven load on the gums and jaw bones provokes early periodontal disease;
- crowding of teeth does not allow them to be cleaned properly and leads to problems with prosthetics;
- the chewing process is disrupted, causing the temporomandibular joints to suffer;
- Snoring appears, apnea (stopping breathing during sleep) may develop.
A carefully performed operation will eliminate all these troubles and significantly improve the quality of life for people with malpositioned lower and/or upper jaws.
Sinus lifting – briefly about the method
When implanting in the lateral areas of the upper jaw, in the vast majority of cases, raising the level of bone tissue is required. The upper jaw is an air-bearing organ. It contains the maxillary sinuses, lined with ciliated epithelium, which is responsible for purifying the air we inhale. The sinus lift operation involves carefully lifting the mucous membrane with curettes and performing bone grafting. In fact, a sinus lift is a version of the GBR for the upper jaw in the projection of the maxillary sinuses. The success of bone grafting for alveolar process atrophy depends on the patient's compliance with doctors' recommendations, strict adherence to the postoperative regimen, non-smoking, and of course, on the experience and qualifications of the operating surgeon!
Indications and contraindications for jaw osteotomy
Corrective osteotomy on one jaw returns it to normal functioning. Surgery on both jaws also improves facial aesthetics.
Indications for its implementation
- improper closure of teeth that is not amenable to orthodontic treatment;
- a clear violation of facial proportions, causing serious discomfort to the person.
Jaw osteotomy should not be performed in the following cases:
- orthopedic or orthodontic treatment has not been completed or not carried out;
- there are any diseases that do not allow a person to be given general anesthesia and guarantee the absence of serious consequences.
The operation should not be performed on people with severe mental disorders or if there is suspicion of malignant cancer.
When is orthognathic surgery not indicated?
The bite can be changed surgically only when the jaw bones are fully mature - that is, only in adults.
Contraindications to surgery are life-threatening conditions or chronic diseases in the stage of decompensation: cardiovascular, endocrine (diabetes mellitus), oncological (especially tumors in the facial area), as well as disorders in the blood coagulation system, some mental illnesses.
Often patients come to us who have a correct bite and harmonious features, but still require surgery and improvement of existing data. Orthognathic surgery, which has truly transformative properties, works, however, only in the presence of real, and not fictitious, problems, and still has limited capabilities, in some ways superior, but also in some ways inferior to plastic surgery.
Sequence of maxillary osteotomy
The orthodontist is the first to treat any malocclusion. Then - dental surgeons.
- An orthodontist installs braces on the upper and lower jaws to straighten the teeth. For some period of time (~9-10 months), because of this, the teeth stop closing.
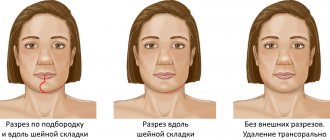
- The patient is given general anesthesia. The incision is made from the palatal side (from the inside of the mouth) so that there is no scarring. Cuts are made on the jaws, bone fragments are set in motion and placed so that the shape of the face is most attractive. The new position of the jaws is secured with small titanium plates, which take root well, do not ring metal detectors at the airport, and allow MRI scans to be performed without difficulty. Most often, the plates remain in the body forever and are not felt at all. The muscles, mucous membranes and other tissues are sutured so that there are no disturbances in the nearest nerve branch, an antiseptic bandage is applied to the wound, and the person is taken to the ward to wake up after anesthesia.
Errors in the treatment of distal occlusion
The first, main mistake is that many try to treat distal bite with one device. For example, only with braces (this is the most popular option). But braces, although a cool device, are not for skeletal problems. The level of hardware competence of the braces system does not extend further than “to place the teeth on the jaw.” And distal occlusion, as we have already said, is a purely skeletal problem. Jaws and posture are to blame. And braces are not capable of solving problems with posture or jaw problems. After all, braces cannot change the position or size of the jaw. No matter what the would-be doctors promise...
And therefore, such videos are just an advertising gimmick.
Or rather, a convenient “hook” that catches gullible patients. Convenient because it coincides with the desire to do everything quickly and efficiently... But it doesn’t coincide with reality.
And braces cannot be the main device in the treatment of distal occlusion.
Braces are the wrong choice when treating distal malocclusions. In any case, you definitely shouldn’t start with them. Braces, as mentioned and shown above, can be effectively used only at the final stage of treatment of distal occlusion. All major “feats” must be accomplished before working on the teeth. Before using braces. And they are accomplished at the level of the jaws and skeleton (posture). Otherwise, there will simply be nothing to “clog” (close) these teeth (read with braces). See “Fundamentals of the therapeutic concept of “Ortho-Arteli”.
The second common mistake in correcting distal occlusion is treatment with the removal of upper premolars (4 or 5 teeth).
And this mistake is much more serious. Because it can have the most dire consequences. See "Orthodontic treatment with tooth extraction."
After all, as we said above, the main causes of distal occlusion are skeletal. And most often the lower jaw is to blame. And if so, then a reasonable question arises: if the lower jaw is to blame, what does the upper teeth have to do with it (their removal). Where is the logic?
In general, all errors in the treatment of distal occlusion in an adult are usually associated with insufficient diagnosis. Which entails a misunderstanding of the reasons for the occurrence of distal occlusion in each specific case.
For example, the “dental” cause of distal occlusion is very often confused with the “skeletal” (jaw) cause. We remind you that in the first case you need to move the lateral teeth back. And in the second - to push the lower jaw forward and develop the upper one. And if you get confused, if you don’t figure it out... Start distalizing the upper teeth, or worse, remove them when it is necessary to advance the lower jaw... Or vice versa. It is clear that nothing good will come of it.
The third mistake is when, without understanding what’s what, what exactly is the cause of distal occlusion, but realizing, however, that the problem cannot be corrected with braces, they try to solve the problem surgically. Using orthognathic surgery. Through osteotomy of the lower and upper jaws.
This is where I would like to dwell in more detail. And explain something. Why do orthodontists send to a surgeon to “treat” a distal bite? They have already said: they understand that braces will not cope. But they don’t understand how to treat it without braces. They don’t understand because in dentistry in general, and orthodontics in particular, there are a lot of prejudices regarding the possibilities of moving the lower jaw forward and developing the upper jaw. And these, as we saw above, are the main (“key”) points in the treatment of distal occlusion.
Most orthodontists simply do not believe in this (that it is possible in principle). Because someone (even a “great one”) said two hundred years ago that this cannot be done. Time has passed. Everyone has already forgotten why it is “impossible”. But no one even bothered to check why, in fact, it was impossible...
And therefore, those doctors who blindly believe in these moss-covered “dogmas” simply do not see an alternative. And for them there are only two extreme poles in the treatment of distal occlusion: braces and surgery. That's all.
During a direct examination by a specialist, you will be able to find out your exact diagnosis, as well as receive a referral for diagnosis or a treatment plan.
And in our clinic we treat distal occlusion between these two poles. Using methods of maxillofacial orthopedics and craniodontics. Here are the ones: changing the position of the lower jaw and changing the size of the upper. And we get good results, without regard to the fact that someone once said something... We must always double-check what was said. We checked. And everything turned out to be somewhat different. Or rather, not at all the way they “frightened” us. You can also push it out. It can be developed. You just need to know how, because there are some “secrets” here. And we, at the Orto-Artel clinic, knowing these “secrets”, take advantage of these opportunities, successfully eliminating distal occlusion of any complexity.
By the way, if we are talking about surgical treatment of distal occlusion, then we need to determine when and in what cases surgery is generally appropriate. But the indication is basically the same - a small lower jaw, the so-called lower micrognathia, and the micrognathia is very pronounced.
We indicated this reason above as one of the skeletal reasons. I will add: the lower jaw should be VERY short. Literally ugly. Only then can this be resolved surgically. In all other cases, you can do without surgery. Proven and tested many times.
By the way... In our clinic, a good half of the patients have formal indications for surgical treatment of distal occlusion. But only a few got to the surgeon. Because formalities are formalities, but compromise solutions were found that satisfied everyone: both the patients and us. This is because we approach treatment not formally, but in essence. And we are guided by logic and common sense.
Well, as a special case of a short lower jaw, which cannot be corrected except by surgery, this is a small chin. If it is small and spoils the face, then even by pushing the lower jaw forward we will not get the aesthetics we want. Simply because orthodontists do not have the means and instruments (devices) to selectively influence the chin. It is impossible to stimulate the chin to grow. Only surgery.
Inferior micrognathia.
This is where the indications (and there is essentially one) for surgical intervention for distal occlusion end.
Going with a knife into the upper jaw - God forbid! Even if the upper jaw is indirectly to blame for the distal occlusion. More precisely, the upper jaw also, as a rule, suffers (dimensionally) with distal occlusion. The upper jaw is directly connected to the base of the skull. And such interventions can then backfire. Literally. And the most important thing is that there is no need to go there surgically. The upper jaw can be developed!!!
Rehabilitation stage
Severe swelling is something all patients should prepare for after an osteotomy. Swelling will persist for up to 3 weeks. Throughout this period, the person walks with rubber bands that prevent the mouth from opening too wide. For nutrition, soft, semi-liquid and warm food with sufficient calories is recommended. Chewing hard foods is prohibited.
After 4 weeks, the patient turns to the orthodontist, who completes the work on the dentition.
Contact only trusted dental clinics; osteotomy is a rather complex type of operation, so it should only be performed by experienced surgeons with good experience.
Potential complications of orthognathic surgery
Detailed computer planning of the intervention and long-term preparation help to almost completely minimize the risk of complications.
After surgery, patients often note temporary numbness of the lips, which, however, has a rather positive effect, since it allows one to avoid pain. Otherwise, any operation carries possible risks, the avoidance of which depends on the professionalism of maxillofacial surgeons and the competent work of orthodontists. Therefore, choose only proven options!