Porcelain crowns for front teeth
The main distinctive feature of porcelain crowns is that they do not contain metal impurities, so their use is especially justified if the patient is allergic to metal. Materials for porcelain crowns are special porcelain-based mixtures that are inert and therefore do not stain or irritate soft tissue.
Just a few years ago, in most cases, prosthetics with porcelain crowns were carried out in the anterior part of the jaw, since it was believed that such products were too fragile for chewing teeth, which bear heavy loads. Indeed, conventional porcelain crowns are more fragile compared to their metal counterparts, but the use of a zirconium dioxide frame made it possible to achieve the necessary strength and make it possible to use them in any area of the jaw. In general, the indications for use of porcelain crowns are almost the same as for other structures of a similar type.
Treatment of a tooth for a crown
The doctor’s task at this stage, like a sculptor’s, is to “cut off all unnecessary” from the tooth, giving it a strictly defined shape. Two things are most important: an even and clear ledge formed near the gum itself, as well as the shape of the tooth and especially the inclination of its walls in relation to each other. These two parameters mainly affect the final quality of the crown and its service life.
The ledge on the tooth is needed so that the edge of the future crown fits evenly onto it. If the doctor does not form a ledge, the edge of the crown will hang between the tooth and the gum, which will inevitably lead to the accumulation of plaque around it, which means inflammation of the gums and tooth caries around this very edge of the crown, and the appearance of an unpleasant odor from the crown. It is important that the ledge is as smooth and even as possible. After all, it is the precise, uniform fit of the edge of the crown to it that is the main factor in the long service life of the restoration.
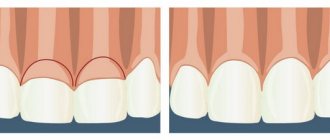
This photo shows approximately what the tooth should look like after the preparation is completed (in this case it is the upper canine). The arrows indicate the ledge on which the edge of the crown will subsequently sit. It is also clearly visible here that the opposite walls of the tooth are almost parallel to each other, and converge at a slight degree (ideally 6-8 degrees).
The shape of the stump after finishing the treatment should roughly resemble the anatomy of a full-fledged tooth (not a Christmas tree, not the roof of a house in a child’s drawing, not a stump or a carnation, but the shape of an intact tooth). This is necessary so that the dental technician can then model a beautiful and functional, i.e. a design that is easy to chew, and not just a flat “table” that can only be used to crush food and not chew. The opposite walls of the tooth should be almost parallel, only slightly converging towards each other. This shape is a guarantee that the crown will serve for a long time and will not disintegrate under the influence of constant chewing loads. If the tooth is “filled with a house”, the tooth stump will be too short - this will inevitably lead first to depressurization of the crown (i.e. it will still stay on the tooth, but microflora from the oral cavity will already begin to get under it), and then to its complete loss.
And here you can clearly see what a tooth should not look like after preparation. The lack of a ledge and too much taper of the tooth stumps led to rapid decementation of the crowns, dental caries and inflammation of the marginal gums...
What other important points are there at this stage? It’s probably worth mentioning once again that when treating living teeth for crowns , the doctor must work with A LOT of cooling. Overheating of the tooth threatens the rapid development of nerve inflammation with all the ensuing consequences in the form of root canal treatment and possible reworking of the crown. Here we can make a small digression on the need for complete removal of nerves in all teeth that go under crowns. The most important thing to remember is that the crown itself is not an indication for tooth depulpation. But this approach, unfortunately, is present in many orthopedists, especially those stuck in the Soviet school of dentistry. Working with living teeth needs to be much more careful and precise, and in general it is more difficult. In addition, there is a chance that a living tooth may become ill under the crown and the structure will have to be removed and probably redone. To protect themselves, first of all, some doctors depulpate any tooth that goes under a crown, indiscriminately. In fact, this is quite definite harm and excess of indications. The main indications are: a strong tilt of the tooth, its protrusion from the dental arch, as well as the presence of deep caries.
Indications and contraindications for the installation of porcelain crowns
| Indications: | Contraindications: |
|
|
Making porcelain crowns
The production of porcelain crowns requires the presence of expensive equipment and experienced specialists on the staff of a clinic or dental laboratory. Today, two methods are used to produce such crowns - layer-by-layer application of porcelain mass and injection molding technology. The second method is considered more modern (as it provides the finished structure with greater strength) and is used in most dental laboratories. The production of a porcelain crown takes place in several stages.
Stage 1 - preparatory
Preparation of teeth for a porcelain crown and selection of color for the future prosthesis.
Stage 2 - taking an impression
The doctor takes impressions of the teeth, which are then sent to a dental laboratory.
Stage 3 - matrix production
Thin platinum foil is used as a mold for the future dental crown, which is placed on the model and filled with porcelain mass.
Stage 4 - firing
The crown goes through several stages of processing under the influence of high temperatures.
Stage 5 - product processing
The dental technician makes adjustments to the structure so that its shape and surface perfectly match the patient’s teeth. At the final stage, the finished structure is painted and glazed.
Clinical aspects of tooth preparation in the manufacture of porcelain veneers
The article is devoted to a practical issue - an algorithm is proposed for the use of abrasive tools in the manufacture of porcelain veneers (porcelain adhesive veneers, hereinafter FAO).
In a number of publications one can find judgments that preparation for veneers is a fairly simple manipulation that does not require significant skill. However, most experts, with whom we completely agree, consider this type of microprosthetics to be a very complex section of orthopedic treatment. Opponents of this point of view would like to object: “If it’s simple, then why such a price?”
Currently, the standards of basic dental education in the Russian Federation do not provide for the treatment of patients with defects in hard dental tissues with veneers. This leads to the fact that young specialists have a very vague understanding of the possibilities of this treatment method and only a few of them are able to qualitatively prepare a tooth for adhesive veneering. Most beginners, trying to impress their colleagues, “treat” patients, ultimately discrediting this type of microprosthetics. In our opinion, this is what leads to the fragility of these structures and prevents their wider use in everyday practice.
I would like to warn my colleagues against some incorrect approaches when treating patients using porcelain veneers. Considering that FAO is most often used to replace defects in the hard tissues of anterior teeth, a certain sequence should be observed. In other words, it is necessary to first replace existing defects in the lateral areas of the dentition, correct occlusal and articulatory relationships, taking into account the characteristics of the bite. It is important to take into account the presence of parafunctions of the masticatory muscles, somatic pathology, and in general all anamnestic data that allows orthopedic treatment with a long-term favorable prognosis.
Your view on the sequence of preparation and the peculiarities of working with abrasive instruments at the clinical stages of manufacturing FAO can be demonstrated using a clinical example of complex treatment of patient K., 55 years old. The primary clinical picture, the sequence of stages of preparation for orthopedic treatment and prosthetics are presented in Fig. 1–3.
Rice. 1. The dentition of patient K. at the stage of preparation for prosthetics.
Rice. 2. Orthopantomogram of the jaws after the manufacture of metal-ceramic crowns and a removable supported prosthesis on the lower jaw with a beam fixation system.
Rice. 3. Dentition after the end of the adaptation period and before the production of FAO for teeth 1.1, 2.1.
The production of veneers should begin only after replacing defects in the dentition and completing the period of adaptation to a removable denture.
As can be seen in Fig. 4, the maxillary central incisors have old composite veneers that do not meet clinical requirements. Unfortunately, dentists rarely encounter clinical situations where a veneer is made on a tooth that does not have any defects or old fillings. Therefore, for demonstration, we chose a rather complex clinical situation, and for clarity of manipulations, a similar tooth preparation was carried out on a phantom.
Rice. 4. Appearance of old direct composite veneers on 1.1, 2.1 teeth.
Anesthesia and opening of the periodontal groove with a retraction thread to ensure good access to the gingival area of preparation and quiet work of the doctor is a necessary condition (Fig. 5).
Rice. 5. Creation of marking grooves to control the depth of preparation of the vestibular surface.
The first stage is the preparation of the vestibular surface of the teeth with the creation of marking grooves that determine the volume of subsequent grinding. Considering that in the classic version, veneers are located within the enamel and their minimum thickness, which gives the porcelain mechanical strength, is 0.6–0.7 mm, marking bur 834-021M-FG is used, the design of the working part of which allows you to create grooves with a depth of 0. 5 mm (Fig. 5, 6).
Rice. 6. Marking grooves (view from the cutting edge).
It is better to apply the grooves in a vertical direction from the area located in the gingival part towards the cutting edge. This stage is important for determining the volume of tissue to be sanded and the thickness of the veneer being made.
The second stage is the formation of a gingival groove 0.5 mm wide and 0.5 mm deep (Fig. 7).
Rice. 7. Creation of a gingival groove with a depth and width of 0.5 mm.
This is conveniently done with a bur 868A-018M-FG with a rounded tip with a diameter of 1 mm, immersing it half the diameter into the hard tissues of the tooth. If you have confident manual skills, you can use burs 881-012С-FG or 882-012С-FG. The level of the groove depends on the condition of the enamel in this area. If the enamel is not destroyed or discolored, it is possible to create a groove up to the gingival margin. You should be very careful to create enough space for the porcelain lining. In other cases, the groove must be positioned more apically, but immersed no deeper than 0.5 mm into the periodontal groove. Insufficient preparation can lead to violations of the “biological width” of the gingival margin and the creation of a hypercontour of the restoration with subsequent negative reactions from the marginal periodontal margin (gingivitis, bleeding, recession).
Subsequent preparation of the vestibular surface can be carried out immediately along its entire plane with the simultaneous creation of grooves on the proximal edges, or first, approximal grooves are formed that connect to the gingival groove (Fig. 8–10)
Rice. 8. Creation of the approximal boundaries of the cavity and preparation of the vestibular surface of the bur.
Rice. 9. Depending on the height of the clinical crown, burs 881-012F-FG or 882-012F-FG are used.
Rice. 10. View of the treated surface from the side of the cutting edge.
Then the hard tooth tissues are ground down along the entire vestibular surface to the depth programmed by the depth marker.
Depending on the height of the clinical crown, burs with different lengths of the working part are used: 882-012F-FG, 881-012F-FG. It should be noted that in any case, when creating the approximal boundaries of the prepared cavity, they must be located as close as possible to the contact points. This allows you to make the edges of the veneer invisible and improve the aesthetics of the microprosthesis. If possible, interdental contacts should be maintained, but given that the edges of the veneer should not be very thin, in order to avoid chipping, the proximal grooves should have a depth of up to 0.5 mm. In some cases, it is necessary to open approximal (interdental) contacts. In our opinion, such preparation transforms the microprosthesis from veneers into the category of half-crowns. In this case, it is necessary to stabilize the teeth with temporary structures to prevent their displacement. In addition, this complicates the laboratory stages of manufacturing prostheses and their subsequent fitting.
Preparation of the incisal edge is the most controversial issue in the manufacture of veneers. Various options are offered: an oblique bevel of the incisal edge, or its thinning, a fenestrated overlap of the incisal edge, or with the creation of an oral sulcus. Thus, two groups can be distinguished: with and without overlap of the cutting edge.
As literature data and our own observations show, the most successful option is with a shortened cutting edge and the creation of an oral groove for strength and reliability of veneer fixation. This should also be taken into account because quite often there are clinical situations when it is necessary to change the length of the cutting edge.
To prepare the cutting edge and create an oral groove, burs 379-023F-FG or 881-012C-FG are used, although only the latter can be used (Fig. 11, 12).
Rice. 11. Shortening the cutting edge and preparing the oral surface, using a bullet-shaped bur 379-023F-FG.
Rice. 12. Creating a groove on the oral surface of the phantom tooth with bur 881-012C-FG.
The final treatment of the cavity is carried out with burs with green markings 882-012C-FG or 881-012C-FG. This achieves the creation of a surface with good characteristics for subsequent adhesive fixation of FAO (Fig. 13).
Rice. 13. Final treatment of the cavity to create a better adhesive bond. Cylindrical burs 882-012C-FG or 881-012C-FG with a round tip and green markings are used.
The final appearance of the formed cavities is shown in Fig. 14–17.
Rice. 14, 15. View of the prepared cavity from different angles, vital teeth before taking impressions.
Rice. 16, 17. ... on a phantom.
Speaking about preparation, we should dwell on some controversial issues regarding the “exposure” of dentin during grinding and the need to make temporary veneers. From our point of view, it is possible to “expose” the dentin to create sufficient thickness of the FAO. In addition, existing modern systems for fixation ensure long-term reliable adhesion to both enamel and dentin.
The production of temporary veneers is mandatory and, due to the availability of composite self-hardening materials for this in the dentist’s assortment, does not cause much difficulty. We made direct temporary veneers (Protemp 4 Garant 3M ESPE) based on the impression taken before preparation. Their temporary fixation is carried out by spot application of adhesive on the contacting surfaces of the provisional veneer and tooth, without etching and with short-term photopolymerization (Fig. 18).
Rice. 18. Provisional veneers were made.
After removing the temporary veneers, we used A-silicone (Expess XT Penta Putty and Ultralight body, 3M Espe) to obtain a working impression, and the veneers themselves were made of low-temperature sintered Noritake ceramics using the Accu Trac system for casting models and obtaining fireproof dies ( Fig. 19–21).
Rice. 19–21. AccuTrac dismountable model system, FAO fitted to the model.
FAO was fixed with Relyx ARC composite cement (3M Espe) of the appropriate shade (Fig. 22, 23).
Rice. 22, 23. Stages of FAO fixation (Relyx ARS composite material, 3M Espe).
In some cases, after fixing the veneer, it becomes necessary to correct its shape from the vestibular surface or in places of contact with antagonist teeth. The first is carried out with a conical bur with a rounded tip 850-014SF-FG, the second with an olive bur 379-023SF-FG, both with yellow markings. In our clinical case, only an olive-shaped bur was useful for shortening the FAO on the left incisor.
Removal of excess material should also be carried out with abrasive tools. It is not advisable to use manual instruments (excavators, probes), as this can lead to marginal chipping of the veneer as a result of uncontrolled pressing on them. For these purposes, we used a carbide finisher H48L-012-FG (Fig. 24).
Rice. 24. Removal of excess material from the cervical area 1.1; 2.1 teeth carbide finisher H48L
012-FG.
If the glazed surface of the FAO was corrected after its fixation, there is a need to treat these areas with ceramic polishing heads. We used aluminum oxide polishers P0362 (Cerapink), P0372 (Cerasupergrey) (Fig. 25).
Rice. 25. Use of ceramic aluminum oxide polishers for polishing areas of veneers ground off after glazing P0362, P0372.
The results of orthopedic treatment of patient K. are presented in Fig. 26–27.
Rice. 26. Appearance of the dentition after permanent fixation of the FAO.
Rice. 27. The result of orthopedic treatment of patient K.
Thus, our recommended set of abrasive instruments for performing the clinical stages of producing FAO includes 11 types of instruments:
379-023SF-FG, diamond bur, oval
Correction of the glazed surface of the veneer at points of contact with antagonists
834-021M-FG, diamond bur, depth marker
Drawing grooves on the vestibular surface to determine the amount of grinding
850-014SF-FG, diamond bur, round tip cone
Correction of the shape of the vestibular glazed surface of the veneer
868A-018M-FG, diamond bur, round tip cone
Creation of the gingival groove
881-012C-FG, 881-012F-FG, diamond bur, round end cylinder
Final treatment of the cavity to create a surface with good adhesion conditions
882-012C-FG, 882-012F-FG, diamond bur, round end cylinder
Creating proximal preparation margins
H48L-012-FG, carbide finishing, flame
Removal of excess composite material after permanent veneer placement
P0362, CeraPink polishers, medium grit
Polishing areas of porcelain in areas where the surface has been corrected after glazing
P0372, CeraSupergrey polishers, fine grit
Polishing areas of porcelain in areas where the surface has been corrected after glazing
All instruments manufactured by NTI-Kahla GmbH Rotary Dental Instruments, Germany
Authors: N. N. Abolmasov, M. S. Serdyukov, S. G. Tyman, O. Yu. Chebotarenko
Porcelain or metal-ceramic crowns?
Much more often we have to compare porcelain and metal-ceramic crowns. Structures with a metal frame have a number of advantages: they are stronger and significantly cheaper. At the same time, they lose greatly in aesthetics: all competent specialists will recommend putting porcelain crowns on your front teeth if you want your smile to be as natural as possible. It is believed that it is justified to install metal-ceramic crowns on chewing teeth, and porcelain crowns on incisors. However, if a porcelain crown has a zirconium dioxide frame, then it can be used to restore any tooth.
Purposes of preparation
In the process of turning teeth for crowns, the following is created:
- Prosthetic space for construction;
- The support stump is of a shape that will provide conditions for the application and fixation of the prosthesis;
- Correct relationship between the edge of the artificial crown and the periodontium.
Each of the above points is very important in the process of functioning of the structure. Prosthetic space is necessary to prevent overbite. The correct shape of the ground tooth will ensure the longest and most durable cementation. And it is worth mentioning separately about the correct interaction with the periodontium.
Price for porcelain crowns in Moscow
The price of a porcelain crown per tooth in Moscow dentistry largely depends on the level of the clinic where the patient is being treated. In most cases, such a design is offered in dentistry at the “business” or “premium” level, where much attention is paid to the aesthetic side of prosthetics. At the same time, the price of porcelain crowns for the front teeth is practically no different from similar designs for chewing teeth.
| Type of dental crown | Price |
| Ceramic porcelain crown | 13,000 - 17,000 rubles |
| Porcelain crown on a zirconium dioxide frame | 19,000 - 25,000 rubles |