Cemental caries, or root caries, is less common than cervical caries, but is considered more dangerous and destructive to the tooth. The fact is that the root walls are thin and therefore caries destroys them faster and reaches the pulp. Root caries often becomes a complication of cervical caries or occurs as an independent disease. Its official name is cement caries, which indicates the location of the lesion - under the gum. This is precisely the problem. Ordinary caries can be seen with the naked eye by characteristic spots, but root caries is invisible.
Different types of caries: WHO classification
Caries is a slowly occurring pathological process in hard dental tissues, which develops under the influence of unfavorable external and internal factors. According to statistics, this disease occurs in more than 90% of people in the world.
In this article
- Different types of caries: WHO classification
- How does dental caries develop in the root area?
- Features of the progression of dental caries
- Dental cement caries - main clinical manifestations
- Diagnosis of cement caries: basic and additional methods
- Treatment of cement caries: main stages
- Prevention of root caries
According to the classification of the World Health Organization, there are several types of caries: enamel, dentin, cement, as well as suspended, other, unspecified caries, and odontoplasia. In this article we will talk about dental cement caries, better known as tooth root caries.
Classification according to the size of the affected area
- Plural form
If acute caries affects more than 5-6 teeth at the same time, then this is called multiple caries. The main causes of such severe pathology are heart disease, kidney disease, respiratory disease and serious infections. In no case should you delay treatment of multiple caries, otherwise you may lose your entire dentition. The disease is equally common in children and adults.
- Single form
In this case, the carious process develops exclusively in one tooth and does not affect its neighbors. The course of the disease is usually very slow and almost imperceptible until it penetrates into the deep layers of dentin.
- Compensated form
This is a chronic caries that develops over years and hardly bothers a person. It causes the formation of many pigmented cavities in dentin.
- Decompensated form
The carious process progresses very quickly; very little time passes from the initial damage to the enamel to pulpitis. It is considered a very complex form of the disease.
Any type of caries, except for extremely advanced cases, is highly treatable. Its essence is to remove corroded tissue, restore the integrity of the walls, disinfect the cavity and fill the tooth. Unfortunately, if pulpitis or periodontitis (complicated caries) has been identified, then removal and further prosthetics may be necessary.
How does dental caries develop in the root area?
A tooth consists of a visible crown, neck and root. The crown is the visible part that is located above the gum. The neck is located lower and covered with soft gum tissue. The area where the root, or cementum, of the tooth is located is the alveoli (the depressions in the upper and lower jaws).
Root caries can develop as an independent dental disease or as a complication of cervical caries. It is considered more dangerous for the tooth because it reaches the pulp faster. With cement caries, the lesion is usually located under the gum, it is not noticeable during external examination, and therefore is more difficult to diagnose.
The main cause of root caries is usually inflammation or gum disease. With this pathology, the gum does not adhere tightly enough to the tooth, resulting in the formation of a periodontal pocket where food debris and plaque accumulate. Gradually it hardens and turns into tartar, which provokes carious lesions.
Other risk factors for developing root caries are:
- cariogenic bacteria in dental plaque are one of the leading risk factors that leads to periodontal diseases (the tissues surrounding the tooth) and, as a result, exposure of the root surface;
- carbohydrate foods that serve as a breeding ground for bacteria;
- insufficient intake of fluoride into the body;
- impaired characteristics of saliva;
- insufficient oral hygiene;
- features of the anatomy of the dental system;
- critical pH (approximately 6.2 - 6.7);
- cervical caries, which gradually moves to the tooth root;
- violation of crown installation technology, as a result of which the gums recede and expose the root.
Some researchers also name low resistance of teeth to carious lesions, endocrine diseases, and diseases of the gastrointestinal tract as possible risk factors for root caries.
Deep root caries is usually called elderly caries because it most often develops in people over 45-50 years of age. This is due to age-related changes in the oral cavity, decreased immunity, and loss of hygiene skills. Together, this leads to the active proliferation of microbes in the oral cavity, which provoke carious lesions of the tooth root.
Classification according to the location of the outbreak
- Fissure caries
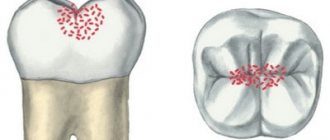
Fissures are called tubercles and depressions on the chewing part of the tooth. They are an ideal place for food debris to stick and bacteria to grow, so cavities are not uncommon there. Fissure caries is always located strictly in the central part of the tooth and never affects its neck and roots. Neglected cavities are usually very deep and painful. If there are no complications, the tooth is filled.
- Contact caries
If the teeth grow crowded, and it is not possible to regularly clean the interdental spaces with floss from stuck pieces of food, then contact caries develops. It got its name due to the fact that the lesion occurs on the proximal part of the tooth. These sides are where the teeth touch each other. The main symptom is the appearance of a dark carious cavity. During treatment, the doctor first restores the side wall and then fills the tooth.
- Cervical caries
The carious process affects the neck of the tooth, it is located near the gingival margin. Here the enamel-dentin layer is very thin, so tartar destroys its integrity in a short time. First, a characteristic white or dark spot appears in the lesion, then the tooth begins to react painfully to sour and sweet foods, as well as changes in temperature. Treatment of cervical caries cannot be delayed, because You can lose a tooth in a short time. Most often, cervical caries affects the front teeth.
- Circular caries
This is a form of cervical caries. They talk about it if the pathological process covers the diseased tooth in a dark ring. Circular caries mainly occurs on baby teeth or is an occupational disease in adults - for example, in musicians who play wind instruments.
Features of the progression of dental caries
In the area of cement, caries can occur in different ways, and on this basis it is classified into 4 types:
- progressive;
- rapidly progressive;
- remission;
- relapse.
Progressive root caries is characterized by a relatively slow rate of tooth root destruction. With rapidly progressing lesions, the lesion spreads in depth and breadth at high speed. The remission stage is when root cement caries does not progress. Relapse suggests that root caries develops along the edges of a previously placed filling.
Caries
Dental caries is a pathological process manifested by demineralization and progressive destruction of hard dental tissues with the formation of a defect in the form of a cavity. This is one of the most common dental lesions, which, according to WHO, affects up to 90% of the world's population. It is observed at any age, but mainly in children and adolescents and equally often in people of both sexes. The teeth of the upper jaw are affected by caries somewhat more often than the lower jaw, perhaps due to the fact that in the lower jaw they are in conditions of better blood circulation and are better cleaned of food debris, which prevents the development of conditions for the occurrence of caries. Caries most often affects the first large molars - molars (from the Latin molares - millstones), since they bear the greatest load during chewing. In second place are the second large molars, in the third are the small molars (premolars) and upper incisors, and in the fourth are the canines. The anterior teeth of the lower jaw are rarely affected. In molars and premolars, caries usually begins on chewing surfaces, in enamel folds - fissures and blind pits, where the enamel layer is much thinner, its mineralization is less pronounced (fissure caries), or on contacting surfaces. Less commonly, the buccal surfaces are affected and very rarely the lingual surfaces. Cervical caries and cement caries are relatively rare.
Etiology and pathogenesis. The cause of caries is still not clear enough. For a long time, localistic chemical and microbial theories of its origin and development dominated and have not lost their importance at present. According to these theories, organic acids, including lactic acid, formed in the oral cavity during bacterial fermentation of carbohydrates, damage the enamel and allow bacteria access to the dentinal tubules. Bacteria penetrating into dentin extract calcium salts from it, soften it, which leads to the destruction of hard tooth tissues.
Microorganisms of the oral cavity are found in greater or lesser quantities in dental plaque, which forms in fissures, pits on the contact surfaces of teeth, around the neck of the tooth under the gum. The formation of plaque has a certain sequence: from the attachment of bacteria to the pellicle (a derivative of saliva contains amino acids, sugars, etc.) and the formation of a matrix to the proliferation of bacteria and the accumulation of their metabolic products. Dental plaque with the formation of dental plaque is currently given a leading role as a local factor in the appearance of the initial manifestations of caries.
Dental plaque also underlies the formation of supragingival and subgingival tartar.
It has been established that microbial associations (streptococci, staphylococci, lactobacilli, etc.) have increased hyaluronidase activity. A direct relationship has been found between the activity of this enzyme, the pH of saliva and the degree of caries development.
It has been shown that hyposecretion of saliva and a lack of parotin (a hormone of the salivary glands) accelerate the development of caries, while an excess of parotin has an anti-caries effect and favors the normalization of protein and mineral metabolism in teeth.
In the origin of caries, not only local chemical and microbial factors play a role, but also the general condition of the body, hereditary predisposition, age - periods of eruption and replacement of milk teeth, puberty. It is during these periods that the greatest caries damage is observed. Of great importance are disturbances in the body's mineral, protein and carbohydrate metabolism, incorrect ratio of calcium and phosphorus salts in teeth, lack of vitamins, microelements, especially fluorine, and hormones. Due to the deficiency of these substances, the activity of pulp odontoblasts with its neurovascular apparatus, which perform the function of intradental trophic centers in relation to the hard tissues of the tooth: enamel, dentin and cement, is apparently disrupted. In the occurrence of caries, one should take into account geographical factors, living conditions, nutritional patterns and other factors affecting the external environment on the body.
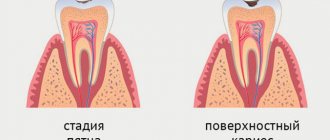
Pathological anatomy . Based on the nature of clinical and morphological manifestations, 4 stages of caries development are distinguished: spot stage, superficial, medium and deep caries. Based on the nature of the course, a distinction is made between slow and fast-flowing caries.
The spot stage is the early stage of caries. The onset of caries is expressed by the appearance of a white opaque spot against the background of the shiny surface of the enamel, reminiscent in color of chalk (chalk stain). The results of morphological and microradiographic studies of dental sections showed that the pathological process begins with dis- and demineralization in the subsurface zone of the enamel. A decrease in the content of calcium, phosphorus, fluorine and other minerals has been established. Initially, calcium salts disappear from the interprismatic substance, and then from the prisms. The spaces between the prisms expand, the contours of the prisms are erased, become fine-grained and turn into a structureless mass. As a result, the enamel loses its uniformity and shine, and later softens. The permeability of enamel increases at this stage.
The chalk spot may become pigmented (yellowish to dark brown), which has not been properly explained. It is believed that pigmentation may be associated both with the penetration of organic substances and their breakdown, and with the accumulation of tyrosine in the spot and its conversion to melanin.
The enamel layers and dentin-enamel junction are not damaged at this stage. The carious process may subside, accompanied by remineralization, and the enamel spot acquires clear boundaries. As caries progresses to the pigmented spot stage, enamel demineralization increases.
Superficial caries is a process of ongoing demineralization and destruction of enamel within the dentin-enamel junction. Calcium salts disappear from the enamel prisms, the interprismatic substance is destroyed, the prisms look more prominent, and transverse striations are clearly visible in them, explained by the uneven dissolution of calcium salts. The prisms are arranged randomly and gradually undergo complete destruction. In areas of enamel defects, microbes accumulate and begin to spread through the loosened interprismatic substance, along the cracks formed between the preserved prisms. With the rapid progression of caries, the process spreads to the dentin; with its slow progression, the softened area of enamel again calcifies (remineralization) and hardens.
Middle caries is a stage of caries progression in which the dentin-enamel junction is destroyed and the process moves to dentin. Dentinal tubules expand, are filled with microbial masses, and the processes of odontoblasts, under the influence of microbial toxins, undergo degeneration and necrosis with disintegration into separate fragments. The membrane lining the inside of the tubules also dies. This facilitates the penetration of microbial waste products into the deeper tubules of dentin and enhances its demineralization and softening.
A carious cavity (hollow) is formed. The carious focus has the shape of a cone, with its apex facing deep into the tooth and its base toward its surface. In the area of the bottom of the carious cavity, three zones can be distinguished. The first is the zone of softened dentin: it completely lacks dentin structure, it is soft, completely devoid of calcium salts, and contains many different microbes. The second is the zone of transparent dentin, this is calcified dentin, its tubules are narrowed, the tissue becomes homogeneous, as a result of which it becomes more transparent compared to the area of unaffected dentin. The third is the zone of replacement (irregulatory, secondary) dentin, which is formed by odontoblasts and does not have ordered tubules. The formation of replacement dentin should be considered as a compensatory reaction (reparative regeneration) that helps stabilize the process.
Deep caries represents a further progression of the process with the formation of a cavity in softened dentin. Between the carious cavity and the pulp, a narrow layer is preserved - the bottom of the carious cavity. In case of destruction (penetration) of this layer, the carious cavity reaches the pulp.
Microradiography data of teeth affected by caries show that at all stages of its development, alternating zones of demineralization, remineralization of enamel and dentin can be observed. The processes of enamel mineralization are carried out mainly due to the intake of mineral salts from saliva. Mineralization increases as it approaches unaffected tissues. In deep caries, the most characteristic features are the formation of an area of increased mineralization at the border of the dentin and the tooth cavity and the abrasion of the pattern throughout the rest of the dentin due to demineralization. It is also important to note that as caries develops, there is a decrease in calcium salts in the remaining hard tissues of the tooth, a decrease in the resistance of enamel and dentin, and a decrease in phosphatase activity in teeth. On this basis, the mechanism of calcium phosphate deposition under the influence of phosphatase is weakened, which contributes to the progression of caries.
In addition to the typical morphological picture of caries described above, there are some variants of its development and course, observed mainly in children and relating to milk or malformed teeth due to calcium metabolism disorders. These include:
- circular caries, starting in the neck of the tooth and covering it in a ring; the course of the carious process is rapid, without the formation of a zone of borderline transparent dentin and accompanied by significant destruction of tooth tissue;
- early, or subenamel, caries develops directly under the enamel layer;
- lateral caries, which occurs on the lateral sides of the tooth, resembling circular caries in terms of localization of the lesion, but differs from the latter in a slower course;
- stationary caries is limited only by the dissolution of the enamel and stops there; found almost exclusively in first molars;
- retrograde caries develops from the pulp, affects dentin and then reaches the surface of the tooth, destroying the enamel.
The microscopic picture resembles the picture of ordinary caries, but in reverse [Abrikosov A. I., 1914]. It is observed with purulent pulpitis of hematogenous origin, with tooth trauma, with dental anomalies in both children and adults.
Cement caries is rare, mainly when the tooth root is exposed and there are inflammatory processes in the periodontium. It is manifested by destructive changes in cement and its resorption - cementolysis. Along with this, an increase in the layer of cement is sometimes observed - hypercementosis.
Complications. A complication of medium and especially deep caries is pulpitis.
Dental cement caries - main clinical manifestations
At an early stage, there may be no symptoms of cement caries at all, making early diagnosis difficult. When a cavity grows, the following symptoms may appear:
- Discomfort while eating.
With root caries, mobility of the damaged tooth is often observed, which causes discomfort while eating. In addition, minor pain can result from food particles getting into the gum pocket or directly into the carious cavity.
- External defects.
If caries spreads from the root upward to the cervical area, during the examination the dentist may detect visible changes in the color and structure of the tooth.
- Pain.
It can appear when the tooth is exposed to cold or hot, or when eating salty, sweet, or sour foods. It is impossible to detect root caries on your own, so you need to visit the dentist twice a year. This is especially important for older people and those with gum disease. In such patients, root caries and deep caries are quite common.
Clinic and diagnosis of enamel caries
The difficulty in diagnosing initial enamel caries in the spot stage is that the patient does not experience any discomfort - the tooth reacts normally to changes in temperature, sweet, sour and salty foods and only in rare cases, for example, if enamel caries develops in the area of the sensitive neck of the tooth, mild discomfort is possible. Visually, enamel caries can appear as a white spot or a small cavity. The tooth surface in the affected area may become slightly rough.
One of the most insidious clinical cases of enamel caries is lesions in the interdental spaces. Since this area is hidden from view, pathology can often only be detected at a later stage.
What complicates the diagnosis of enamel caries is that damage to tooth enamel is not always caries. Fluorosis, erosion, abrasion of enamel and hypoplasia have similar symptoms. For example, both fluorosis and hypoplasia are accompanied by white spots or roughness on the enamel.
Types of diagnostics
- Visual examination
in the clinic using drying - this allows you to detect a rough surface on smooth enamel. - Diagnosis
of caries on tooth enamel using dyes: a quick and easy way to determine whether a patient is developing caries - or if it is just pigmentation. The fact is that with initial caries, tissue softening occurs in the enamel, and if the lesion is carious in nature, the dye will easily penetrate into the affected tissue and color it. With fluorosis or hypoplasia, staining will not occur. - Fluorescent diagnostics:
exposure of teeth to special ultraviolet lamps, during which healthy tissue begins to glow with a bluish or greenish light, but in the area affected by carious bacteria there is no similar effect. The method is quite accurate, but expensive.
Diagnosis of cement caries: basic and additional methods
Diagnostic methods that help identify dental caries are divided into basic and additional.
The main ones include:
- patient interview;
- external visual inspection;
- probing - determining the depth of the cavity, as well as the density and tenderness of tissues, using a dental probe;
- percussion (tapping on the tooth).
Additional diagnostic methods are:
- staining with a special dye to see the affected areas;
- thermal test - the tooth is irrigated with cold water and the pain reaction is assessed;
- radiography - helps to detect hidden carious cavities and caries of contact surfaces;
- electroodontometry - prescribed to determine the condition of the pulp;
- luminescent method - illumination of teeth with ultraviolet rays, under which tissues affected by caries change their shade.
Root caries itself is most often diagnosed through sequential manipulations:
- remove deposits from under the gums using ultrasonic and manual instruments;
- isolate the tooth root from saliva using a special plate;
- using a probe, assess the condition of the root surface;
- with the help of x-rays or radiovisiography, even small defects under the gum, in the gingival zone, and carious lesions at any stage are detected;
- if necessary, confirm the diagnosis of “cemental caries” or differentiate it from pulpitis, thermometry or electrical odontometry is prescribed.
Indications and contraindications
Indications for treatment of the disease are both visual and tactile; these include:
- color change, enamel pigmentation;
- painful reaction to hot or cold, sweet or salty;
- enamel chipping;
- darkening of the cervical segment;
- carious cavity;
- a dark gap located along the border of the filling.
There are also contraindications to caries treatment:
- acute respiratory diseases;
- first and third trimesters of pregnancy;
- acute stage of periodontal disease, which is accompanied by severe bleeding of the gums;
- herpes in the acute stage.
Treatment of cement caries: main stages
With root caries, the most difficult task is to gain access to the affected area, especially if the carious lesion is located under the gum. Traditionally, treatment of root caries takes place in several stages:
- Retraction. First, the dentist artificially exposes the neck of the tooth and part of the root, lowering the gums with special devices.
- Coagulation of the gums. It is carried out if indicated using laser exposure to gum tissue. The essence of the manipulation is to remove overgrown tissue.
- Direct treatment of caries. The choice of tactics depends on the degree and depth of the lesion. If caries is in the initial stage of the stain, then remineralizing therapy will be sufficient - restoring the mineral composition of tissues with the help of fluoride preparations. If the doctor reveals more extensive and deep caries with the formation of a cavity, then surgical treatment with preparation and filling will be required.
- Installation of an inlay or crown if the volume of destroyed tissue is more than 50%.
It is necessary to treat cement caries only in a trusted clinic with a reliable specialist, since violation of treatment technology and the use of low-quality materials can cause secondary caries, provoke the development of infection and inflammation of the gums, and lead to tooth loss.
Symptoms of caries
With all the variety of types of caries, its signs are approximately the same and depend on the degree of demineralization and penetration of carious microbes deep into the dental tissues.
- Spot formation. The appearance of a patch of demineralized enamel on the surface of the tooth. Its structure is broken. At this point, the problem can be solved by simply replenishing the mineral deficiency in the area of the stain. Nothing bothers the person, and the white spot can be detected by staining with methylene blue.
- Superficial caries affects the enamel of the tooth, and middle caries affects the dentin. Typical symptoms include dark cavities in the crown, slight pain during brushing, and increased sensitivity to hot, cold, sweet and sour foods. To prevent caries from progressing to medium or deep, you need to urgently undergo treatment for superficial caries.
- Deep caries is often quite painful, and sometimes the pulp is separated from the cavity by only a thin layer of dentin. Acute pain occurs when there is a sudden change in temperature or exposure to chemical or mechanical irritants. When they are eliminated, the unpleasant sensations immediately disappear.
- If the pain continues for hours and occurs when chewing or the slightest touch to the tooth, it means that caries complications have already developed - pulpitis or periodontitis. These are very unpleasant and dangerous diseases that require serious treatment.
At the initial stage, caries can only be recognized by a dentist. This is why it is so important to visit a doctor for a preventive examination at least twice a year. Spend just half an hour on a visit, and caries treatment will consist only of tooth remineralization. Agree, maintaining a healthy smile is so easy if you spend a little more time on it!
Prevention of root caries
The following preventive measures will help reduce the risk of root caries:
- Maintaining oral hygiene. In addition to brushing your teeth, it is important to pay increased attention to careful and thorough gum care and high-quality cleaning of periodontal pockets. For this purpose, it is convenient to use irrigators, which with a powerful stream of water remove food debris even from under the gums, massage the gums, helping to strengthen them.
- Timely treatment of gum disease, as this is one of the main causes of root caries.
- A rational and balanced diet with a minimum amount of fast carbohydrates and a large amount of vitamins and minerals.
- Limited consumption of hard foods that can injure the gums.
- Regular visits to the dental clinic at least twice a year.
Following simple preventive measures will help prevent root caries and maintain dental health even in old age.
Modern methods of treating dental caries
In our dentistry, caries treatment is carried out using the latest methods. The priority issues of modern therapy are restoration of aesthetics, functional state of the unit, prevention of migration of inflammation to pulp tissue:
Treatment of caries without the use of a drill
:
- infiltration
_ Treatment of caries without drilling is practiced at the initial stage and involves chemical-mechanical treatment. A special gel is applied to the working area of the tooth to break down the enamel. The bacterial focus is dried under the influence of a stream of air and ethyl alcohol, and treated with polymer resin. Advantages of caries treatment without drilling: non-invasiveness, atraumaticity, speed of therapy, preservation of the unit’s shape, restoration of fluorescence in 80% of cases. Correction of pigmented spots allows you to stop the demineralization process and save the tooth; - air abrasive polishing
. The surface defect is “knocked out” by an intense flow of abrasive ingredients, while only areas affected by microorganisms are affected. In terms of efficiency, the method is comparable to using a drill and drilling, does not require freezing, and minimizes the risk of microcracks; - ART method
. Restorative therapy, which involves high-quality removal of pathology followed by filling the affected area with dental cement without the use of special equipment; - laser correction
. Used to eliminate the focus of caries through fluorescence. The laser acts precisely on the problem area, “evaporates” it, and at the same time disinfects the resulting space, which minimizes the likelihood of relapse; - remineralization
_ Turnkey treatment of caries is carried out according to the following scheme: professional sanitation of the oral cavity - selection of individual hygiene products - remineralizing therapy using a solution of calcium gluconate, fluoride-containing drugs. After completing the course, there is a stabilization of the balance of minerals in the oral cavity and an increase in the stability of the enamel.
Treatment of caries using preparation
In advanced cases, non-invasive methods of medical intervention, for example, treatment of caries without drilling, do not produce results, so doctors practice mechanical cleaning (preparation) of the deformed area. When dentin is damaged, infected tissue and pulp are removed.
Modern specialized devices allow you to perform all manipulations quickly, painlessly, and as comfortably as possible for the patient. After preparation, a filling or restoration is installed.
Stages of invasive treatment of advanced caries:
- preparation: cleaning from plaque using special tools, selecting the shade of the filling material;
- local/general anesthesia;
- preparation;
- medicinal treatment with a solution of cobalt chloride, application of a paste containing calcium hydroxide;
- installation with a calcium-containing gasket. Has a bactericidal and remineralizing effect, promotes tightness;
- placing a filling with regeneration of the tooth shape;
- polishing, grinding the filling.
For your information …
Oral diseases are dangerous because they can occur with complications and ultimately lead to a deterioration in the health of the body as a whole. The most common and well-known diseases are gum disease and caries. Gingivitis (lat. gingivitis) - inflammation of the gingiv (gums) and caries (lat. caries dentis) of teeth most often owe their occurrence to facultative microflora (microbial deposits, bacterial processes), which manifests itself with inappropriate oral hygiene. Pathological processes (complications of the initial stages of diseases) can be caused by exogenous and endogenous factors of the state of the body as a whole. Exogenous (external) causes are viral or infectious diseases that result in a weakened immune system. Endogenous (internal) causes are chronic diseases of internal organs or hormonally caused changes in the body (pregnancy), which result in hormonal imbalance, metabolic disorders, etc. An important role is played by the structure of the jaw system and dentition (bite), as well as hereditary predisposition.
Treatment of deep tooth root caries
Patients who were not lucky enough to receive such a diagnosis want to know: is it possible to treat tooth root caries and what is done to eliminate tooth root caries? The answer to the first question: yes, this disease can and should be treated. On the second, treatment tactics depend on what stage the pathological process is at, how many units it has affected and at what speed it develops. To ensure that the measures taken give the best result, CELT dentists take into account the condition of the patient’s oral cavity, as well as the presence of concomitant diseases.
Remineralization
This method can only be used at an early stage of caries development. It is aimed at influencing cement and dentin with preparations that contain sodium or tin fluoride, or calcium preparations, as well as antiseptics. They are used during applications to stop the pathological process due to the remineralization of dental tissues. In the vast majority of cases, the technique gives good results, since the porous structure of the cement absorbs drugs well.
Preparation
If the diagnosis reveals damage to hard tissues and a violation of the boundary between cement and dentin, the following measures are taken:
- Local anesthesia;
- Opening a carious lesion;
- Preparation of healthy dentin (practice with rapid progression of the disease);
- Careful removal of softened dentin tissue;
- Formation of a cavity for filling;
- Carrying out filling with a material that is not susceptible to moisture.
The latter is due to the fact that the filling area is located near the gum and the gingival fluid can destroy the normal material. The patient may receive a recommendation to visit a dental surgeon: the latter will perform an intervention and cover the exposed root with a gum flap. This is important because cement effectively protected by gum tissue will not be susceptible to the negative effects of bacteria and acids.
After treatment, the patient needs to regularly and correctly carry out oral hygiene measures. They will eliminate the risk of relapse of the disease and the development of secondary caries around the cavity that was filled. You should not only brush your teeth, but also use dental floss twice a day after meals. In addition, it is recommended to rinse your mouth with alkaline mineral water after consuming sweets, including fruits.