Progeny is a deviation from the norm in the structure of the dentition. It is expressed in enlargement and protrusion of the lower jaw. Such pathological deformation occurs statistically in the range of 1.4 - 30% of patients.
External signs:
In addition to a protruding lower jaw, patients with pathology experience:
- recession of the face in the middle part;
- thickening of the lower lip relative to the upper, its protrusion, and sometimes inversion;
- deepened nasolabial folds;
- increased angle between the lower and upper jaw.
Why is progeny dangerous?
With progenia, the process of chewing, digesting and assimilation of food is disrupted. A person with a severe pathology experiences difficulty while eating, sometimes even cannot take a full bite, which leads to increased stress on the gastrointestinal tract.
There is a redistribution of the load on the teeth, as a result of which some of them wear out faster and require frequent treatment. In addition, the proportions are disrupted and the appearance of the face changes. Such an aesthetic defect in childhood can cause complexes and isolation in a child.
Impairments in oral breathing also appear. The consequence of this is an increased incidence of colds, periodic chapping of the lips and dryness of the oral mucosa.
Causes
What are the causes of such malocclusions and are they only the lot of the elderly? In fact, progeny can begin to develop at any age; pregnant women are especially susceptible to it due to taking certain medications. Also reasons are:
- genetic pathologies;
- injuries;
- congenital cleft palate;
- dental abnormalities;
- loss of teeth for various reasons;
- pathology of the alveolar processes.
Classification of progeny
Pathology is divided into false and true.
In cases of true progeny, the lower jaw develops to a greater extent. In patients with this type, diction is impaired and all external signs of pathology are present. The appearance is influenced by genetic factors, birth injuries and diseases of the woman during pregnancy. It is important to begin treatment at an early age, while the maxillofacial bones can be corrected. Corrective measures are limited to delaying the development of the lower jaw, using massage, and sometimes surgical intervention. In adulthood, adjustments are more difficult. You will need surgery and wearing an orthodontic device.
False progeny is characterized by normal jaw size. In this case, the lower one is shifted forward. Such a bite is formed when a person has to push it forward, as a result of which the muscles and ligamentous apparatus develop incorrectly. The causes are prematurely lost or removed milk teeth in the upper jaw, delayed replacement of teeth, or constant fixation of the lower facial region in the wrong position.
Mesial occlusion (true and false progeny, progenic relationship of the anterior teeth)
To treat progeny in preschool children, E.I. Gavrilov and G.A. Turobova (1965) developed a myofunctional complex, which includes 5 special exercises:
- grasping the lower lip with the upper teeth and upper lip; with the mouth half open, the child places the middle and index fingers of both hands on the chin and, on the count of “1,2,3,4,” when closing the mouth, as if pushing the lower lip under the upper lip and teeth; then he lowers his hands and, at the count of “1,2,3,4,” holds his lower lip without using his hands, rest for 2-3 seconds. and the exercise is repeated 3-4 times;
- exercise with a wooden stick, which is made of durable wood (birch, beech) and should have the following dimensions: width = the width of 6 front teeth, length for ease of holding at least 10 cm, thickness = 3-4 mm, sterilize the board by boiling.
Methodology: the doctor takes a stick in his right hand and places it between the cutting edges of the upper and lower front teeth, the child’s head is slightly thrown back and lies on the doctor’s left hand, the child closes his jaws tightly, and the doctor, without applying much force, moves the stick from a horizontal position to oblique, pushing the lower jaw backward; in this case, care must be taken not to injure the mucous membrane of the palate; the duration of the exercise is 1-2 minutes, after adaptation - 3-4 minutes; at the beginning of classes, some children may have mild, quickly passing pain in the joint; the stick is essentially a short-term inclined plane; closing the mouth with moving the lower jaw back with the help of a doctor: the child’s head is slightly thrown back and supported by the doctor’s left hand, who asks him to open his mouth slightly, then puts his right hand on his chin and, while slowly closing his mouth, moves it to the count of “1,2,3,4” lower jaw back, trying to bring the front teeth at least to direct closure, rest for 2-3 seconds. and repeat 3-4 times; moving the lower jaw back with the help of the tongue - for older children: the child is asked to open his mouth and raise his tongue upward and backward, then on the count of “1,2,3,4” he is asked to slowly close his mouth, while moving the lower jaw back to the ratio of the teeth “butt”, then to the starting position, duration 1-1.5 minutes; repetition of the first exercise
The entire complex lasts 8-10 minutes from start to finish, but some children get tired after 2-3 minutes. Exercises should be carried out regularly 2 times a day: in the morning before games and after naps.
The child is offered a uniform opening of the mouth, which should be controlled by pressing the palms of the hands on the side surfaces of the face. With the palms of the hands, the patient feels possible deviation or asymmetrical movement of the articular heads, which he should avoid. Over time, when the movements become sufficiently coordinated, the patient can control the symmetry of movement in front of the mirror without manual pressure.
In children who cannot independently control the symmetry of the movement when opening their mouth, parents can be encouraged to do this. The mother (father or other relatives) should place the thumb on the chin and the index finger below and evenly open and close the mouth. After several combinations there is no need for parental control. It is very important when carrying out these exercises to eliminate blocking points that delay the movements of the lower jaw. For this purpose, it is necessary to grind off the unworn cusps of baby teeth, fillings or dentures after analyzing the occludogram.
If the upper jaw is underdeveloped, it is recommended to massage the alveolar process from the vestibular side and from the oral side for 2 minutes 2-3 times a day. It is especially effective at the age of 6-7 years.
Treatment of true progenia (lower macrognathia) or false progenia (upper micrognathia) only with intraoral devices only leads to the correction of the dentition or individual teeth, a change in their inclination and partially alveolar processes. The combination of intraoral devices with long-term use of a chin sling with a rubber traction to the head cap, which is also a preventive measure, is more effective and allows, if possible, to normalize the growth of the jaws during the period of milk teeth and mixed dentition. Rubber traction and a rigid chin sling restrain the growth and displacement of the lower jaw.
This method can be used independently or to enhance the effect of intraoral orthodontic appliances. This method has a number of advantages: short application time, longer time intervals between control examinations, no damage to the mucous membrane of the oral cavity and teeth, support in the back of the head or neck makes it possible to apply significant forces without the risk of resorption of the roots of the teeth being moved.
The force of elastic traction should be adjusted, starting with small values (~ 150-200 grams at the chin), with a gradual increase over 2-3 months to 400-450 grams, and then to 700-750 grams. The direction of action of the rubber traction (vector of forces applied to the lower jaw) should be oriented along the line from the mandibular symphysis (progion point) to the mandibular head. When the anomaly is combined with an open bite, it is necessary to add a vertical component of traction.
To make a rigid sling more accurately, the pogonion point is marked on the skin of the chin with a chemical pencil, and the direction of traction and boundaries are marked with an arrow, which, when an impression is taken from the chin, is transferred to it and then to the plastic. Some patients, when wearing a hard sling, complain of a feeling of sweating and skin irritation at the points of contact. To prevent this, the inner surface of the sling can be covered with an adsorbent (talc), a piece of soft cloth, or several small holes can be made in the sling. The boundaries of the chin sling should also be considered. When protruding the lower anterior teeth, it is desirable that its upper border reaches the red border of the lips, and the lower border overlaps the lower edge of the jaw 2-2.5 cm posteriorly. It is recommended to end the side edges of the sling at the level of the corners of the mouth.
Clinical observations have shown that such treatment can begin as early as 1.5-2 years of age. A necessary condition is dosed, regular and long-term use of the sling, at least 9-11 hours a day, for 2-4 years. Treatment should not stop during the retention period. Such a patient should be registered at the dispensary and especially carefully observed during the “critical” phases - the period of teething and puberty, when the growth impulse of the lower jaw may again appear.
Under the action of the chin sling, posterior (counterclockwise) rotation of the lower jaw occurs. In this regard, the growth of the articular condyle slows down somewhat and the position of the mandibular ramus becomes more vertical in relation to the base of the skull. In this case, the chin deviates slightly posteriorly, the Spm point moves, as a result of which the angles SN/Spm and SsN/NSpm decrease. And as a result of changes in occlusal relationships, the upper jaw rotates in the same direction and the SN/SpP angle becomes more open.
In primary occlusion, various devices are used to correct the position of the upper and lower front teeth, operating functionally, mechanically and in combination. With a small incisal overlap, you can use a removable plate with protracting springs or with a sectoral, Y-shaped cut. In case of deep incisal overlap, devices with an inclined plane can be prescribed: Schwartz mouth guard, Bynin mouth guard, Bruckle device.
In the treatment of initial forms of progeny arising as a result of bad habits of sucking a finger or upper lip, it is possible to reduce the sagittal discrepancy of the dentition or even eliminate it using vestibular plates in combination with grinding of baby teeth, especially canines. This is best achieved during the eruption of the first permanent molars and incisors.
Making a vestibular plate is not difficult. Based on the impressions, models are cast and wax bite ridges are prepared. Then the constructive bite is determined, that is, the position is fixed with the lower jaw displaced distally and the models are plastered into the occluder. Wax is layered on the vestibular surface of the upper dentition and alveolar process to the transitional fold, while leveling the sagittal step between the cutting edges of the upper and lower incisors. Using control models, the quality of manufacture of the wax reproduction of the plate is checked, which should fit tightly to the vestibular surface of the lower incisors and be spaced from the upper ones at the distance necessary for their movement. Then the plastic is polymerized according to the usual method.
When treated with such a device, it is almost impossible to breathe through the mouth, and therefore children who are accustomed to mouth breathing may suffocate. To prevent this, several holes with a diameter of 7-8 mm should be made in the plastic at the level of the closure of the lips. As treatment progresses and breathing changes, they can then be covered with self-hardening plastic. Gradually, due to the adherence of the plate to the vestibularly deviated lower incisors, their oral displacement occurs under the action of the orbicularis oris muscle and the plate begins to rest against the teeth of the upper jaw, preventing its growth. In this case, it is necessary to remake the prosthesis or adjust it with self-hardening plastic.
If the mesial bite has developed as a result of displacement of the lower jaw, then after 3-4 months it can be eliminated, but if due to underdevelopment of the upper jaw, then the treatment process is much slower. In the first case, progeny is often combined with a deep bite and deep incisal (more than 4 mm) overlap. In such patients, the Brückle apparatus can be used. The latter represents a base plate for the lower jaw with clasps for the last molars, an inclined plane for the upper incisors, and perhaps a vestibular arch in the area of the lower incisors if their retrusion is necessary. This device is manufactured as follows. Models are obtained from the impressions, clasps are prepared and they are glued to the model with wax. Then the base and inclined plane are modeled, taking into account that it should overlap the cutting edge of the lower incisors by 1/3 of the crown height.
The constructive bite is determined (that is, the one that is planned to be obtained as a result of treatment), the inclined plane is corrected, taking into account the imprints of the palatal surface of the upper incisors to be moved. In this case, the angle of the inclined plane to the occlusal surface should not exceed 45-50°, since at a small angle “thrusting” forces predominate, and too steep an angle contributes to the formation of a deep bite.
If retraction of the lower incisors is required, a vestibular arch is first prepared for them. For this purpose, the lower front teeth to the entire height of the crown, as well as the upper half of the alveolar process, are covered with cement on the lingual side (to create space for their future movement). The device is polymerized according to the usual method and placed in the oral cavity, teaching the patient how to use it, recommending eating soft food for a week. It is better to use the device in combination with a chin sling with a rubber rod to the head cap. At the age of 3.5-4.5 years, this device can quickly change the direction of the axes of the upper and lower incisors.
After the vestibular deviation of the upper incisors by the required amount, the inclined plane is removed, leaving the device as a retention device. If the oral movement of the lower incisors is insufficient, the plastic on the surface adjacent to them can be ground off. The patient should use the device until the lateral teeth come into contact, but at the same time, in the anterior section of the plate there should be a bite pad for the lower incisors, taking into account the amount of incisal overlap achieved. This device can also be used in adults.
An approximately similar mechanism for the treatment of mesial occlusion occurs when using the O.M. apparatus. Basharova (1971). It also represents a base plate on the lower jaw, not adjacent to the alveolar processes and crowns of the incisors and canines. In the front section of the plate there are reversible metal bands (dental retractors) made of stainless steel sheets, 0.4 mm thick, 4-5 mm wide and 60-70 mm long, which are fixed in the base at a right angle.
These metal bands form a kind of inclined plane, and the lateral teeth are separated. Metal bands should not touch the cutting edges and lingual surface of the lower incisors and canines and should be spaced ~3-4 mm from them. The ends of metal strips are brought onto the labial surface of these teeth, onto which a retraction vestibular arch with U-shaped loops is applied. In this device, metal strips can be adjusted to move each tooth individually, while the force of muscle contractions is transmitted through them to the upper front teeth, ensuring their vestibular movement. At the same time, the lower teeth move orally, since the tapes are spaced 3-4 mm from them.
To retain the results achieved during the active period of treatment by O.M. Basharova developed a bite former, consisting of a plate for the upper jaw and a guide plane in the form of wire bends. This guide plane is made from orthodontic wire 0.6 mm thick for baby teeth and 0.8 mm for permanent teeth. Using round-nose pliers, make 6 bends 5-10 mm high and 3-4 mm wide. If the upper jaw is narrowed, an expansion screw can be installed in the base plate.
Treatment of progeny is more successful during the period of mixed dentition, when the lateral teeth have not yet settled into a stable abnormal position. On the other hand, the advisability of early treatment is determined by the fact that each case of progeny, due to the unfixed position of the lower jaw, is aggravated and treatment becomes more difficult.
In orthodontics, due attention should be paid to the health of the nose and larynx. Various pathological processes in them have a certain influence on the formation of dental anomalies. Conversely, malocclusions (progenia, narrowing of the upper jaw, open bite) adversely affect the conditions of physiological respiration. As you know, nasal breathing cleans, moisturizes and warms the inhaled air. So, for example, if the inhaled air has a temperature of 21.7°, then while it reaches the larynx through the nasal passages, it warms up to 30.8°.
At the end of the mixed dentition and in the permanent dentition, guide crowns can be used according to A.Ya. Katsu. The indication for their use is deep or medium incisal overlap, if there is space in the dentition, and with deep overlap, it is better to solder the inclined plane closer to the cutting edge, with less overlap - closer to the neck of the tooth. Crowns are placed on unprepared teeth and do not go under the gum.
The inclined plane is made of wire loops that extend from the cutting edge and from the side surfaces of the artificial crowns of the teeth being moved. The lateral “wings” of the wire loop lie on the palatal surface of adjacent teeth, which allows you to move a group of 2-3 teeth using one device. Inclined plane wire loops are easily formed along the labial surface of the lower teeth, forming the correct fit and contact with them. The amount of movement of the lower teeth can be adjusted depending on the length of the linear contact and the angle of inclination, and the “grid” allows this to be controlled.
If there is no gap in the dentition for the tooth to be moved, then guide crowns with expanders are used. When progeny, two guide crowns are used, fixed on the upper inclined plane, the lateral upper incisors are captured, and the loops overlap the cutting edges of the six anterior teeth of the lower jaw (from canine to canine). Contraindications in primary and mixed dentition may be tooth mobility or small incisal overlap (minimum acceptable - 2 mm). Failure to do so may result in complications such as an open bite.
The R.Fränkel type III function regulator in combination with a chin sling, therapeutic exercises and speech therapy classes has a reciprocal effect: it allows you to stimulate the growth of an underdeveloped area of the upper jaw and retard the growth of the alveolar process of the lower jaw. When there is mesial shift of the mandible, the function regulator, although bulky, is more useful than a facebow.
The action of the regulator, in this case type III, is based on achieving myodynamic balance, that is, on the principle of eliminating the pressure of the lips and cheeks on the alveolar process and dentition in areas of their underdevelopment, normalizing the position of the tongue, and closing the lips. For the treatment of false progeny (mesial occlusion due to underdevelopment of the upper jaw), FR - III is used, the design differences of which from others are that pelota are placed in the upper lip area, a vestibular arch is made for the lower anterior teeth, a palatal arch is made for protraction of the upper anterior teeth , and on the lateral teeth - occlusal pads to separate the bite.
Clinical and laboratory manufacturing stages: impressions are taken, paying special attention to the topography of the transitional fold, models are cast and wax templates with bite ridges are prepared. In the clinic, a constructive bite is determined, for which it is recommended to move the lower jaw back and set the front teeth, if possible, in marginal closure, that is, “end-to-end”, after which the models are plastered in an occluder. Then, in the area of the upper frontal teeth, where the pelota will be located, the model is engraved on both sides of the frenulum, deepening the transitional fold by 5 mm, since on the impression and model it always appears in a somewhat stretched form. Part of the plaster is also removed along the transitional fold at the level of the apical base in the area of the upper canines and first premolars, without changing the direction of the slope of the alveolar process.
When opening the mouth, the lip pads move downwards, which must be taken into account in order to avoid injury to the mucous membrane, so the pads and cheek shields should be 2-2.5 mm away from the alveolar process. For this purpose, a wax pad is placed on the model in the shape of these elements. A spacer is placed on the lateral teeth to separate the bite.
The bracket connecting the pelots is made of orthodontic wire with a diameter of 0.9-1 mm and its ends are bent in a zigzag for better fixation in the pelots. They should be at a distance of 20 mm in the horizontal direction and spaced 10 mm vertically from the gingival margin. The ends of the wire parts fixed in plastic should be 0.75 mm from the surfaces of the shield inside it.
The clamp is secured to the model with sticky wax. Parts of the wire parts that are free from plastic should be ~1.5 mm away from the mucous membrane and, if possible, should be placed in the natural recesses of the alveolar process, this is especially important in the area of the corners of the mouth, so as not to injure the mucous membrane. The paired parts connecting the lip pads to the cheek shields are placed 1 mm above the ends of the bracket, parallel to them, and then with a downward bend, which is done so that the shield does not rotate.
The vestibular arch of the mandible should adhere to the lower anterior teeth, restraining their vestibular deviation and jaw growth. It is placed horizontally at the level of the apexes of the interdental papillae. In the area of the distal surface of the fangs, bends are made at right angles downwards on the arch. Wire pads are bent onto the lower molars and covered with plastic on top to prevent the molars from moving forward. After polymerization, the function regulator is inserted into the oral cavity, lightly pressing against the lower jaw, which the patient must move backward and close the teeth.
The best results when treated with this device are achieved at the age of 6-8 years. As for true progeny, even long-term use of a function regulator does not eliminate the overdeveloped basal part of the lower jaw.
In case of pronounced dentoalveolar combined forms of progeny, with violation of the dimensions of the apical bases of the jaws, arc devices are used, including the edgewise technique with intermaxillary traction. An arch designed for vestibular deviation of the front teeth is placed on the upper dentition, and a sliding arch is placed on the lower dentition for their oral inclination. Hooks are soldered to the upper arch in front of the thrust nuts by 4 mm, “looking” distally, and similar hooks in the canine area, “looking” forward, are soldered to the lower arch. To eliminate reverse incisal overlap, simultaneously with the Angle apparatus, it is recommended to use a plate for the lower jaw with an inclined plane in the anterior section. For the purpose of oral inclination of the lower incisors, the thrust nuts are moved mesially on the lower arch by 2 mm by rotating them clockwise and creating a gap between them and the tubes into which the ends of the arch are inserted.
To move the first permanent molars mesially with the help of intermaxillary traction, elastic rings are hooked onto the posterior ends of the tubes, and on the lower arch onto the hooks located in the canine area.
Edgewise technique is used in the treatment of gnathic or combined forms of progeny. The standard apparatus consists of rings with locking devices - tubes, fixed on the supporting molars, and braces glued to the remaining teeth located in front. First, round arches of the smallest diameter or twist-flex (woven from several wire threads) are inserted into the grooves of the braces. During the treatment process, twist-flex and nitinol arches are also used, and at the end of treatment, tetrahedral arches of various sections are used, which are strengthened with a ligature or special elastic rings on the “wings” of the braces. During the treatment, the teeth are moved body-wise along a tetrahedral arch, which prevents their rotation.
It is possible, or even preferable, to use the straight arc technique with sequential change of other arcs. At the stage of using a square or rectangular arch, an intermaxillary elastic traction from the lower canines to the upper molars is recommended. The most important element is also a facebow with force traction in the occipital region, but this requires strict control of the magnitude of the force and radiological control to prevent complications from the temporomandibular joints. If treatment is accompanied by the removal of individual teeth in the lower jaw, then elastic chains or closing springs can be used to shorten the dentition.
Face masks of various designs with forehead, zygomatic, chin and other plastic overlays, as well as with metal pins connecting these overlays, are used in combination with non-removable orthodontic devices (Nord, Derichsweiler) for accelerated opening of the median palatine suture or with edgewise technique for “pulling” the upper jaw forward and according to indications in the vertical direction with the help of elastic rings, strengthened in the oral cavity on a fixed apparatus and outside the oral cavity on an extraoral apparatus - a mask. An intermaxillary elastic traction can be used, especially with a medium or low basal angle.
Well-known authorities in orthodontics believe that when treating children with progeny (mesial occlusion) during the period of primary and early mixed dentition, the best results are achieved by using a facial mask.
A method has been developed for the treatment of mesial occlusion using the direct arch technique using the “Utility arch”, that is, a bypass arch: at the initial stage, as a rule, all leveling tasks are performed, that is, aligning the position of the teeth and bringing them to a single occlusal line of the dentition.
If the dentition is significantly narrowed, you can use a palatal expander - a 4-loop clasp. Subsequently, at the stage of correcting the position of the teeth, the round orthodontic wire arch of 0.41 or 0.46 mm “Ortonite” is replaced with a square or rectangular one (0.46 x 0.46 or 0.43 x 0.64 mm) from the same alloy. This working arch corrects the position of the teeth, taking into account their mesiodistal and vestibulo-oral inclination (angulation and torque) included in the brace program.
It is worth noting some features of orthodontic treatment for adolescents and adults. They often experience pain in the area of the teeth being moved, in the first 2-3 days after the application of the appliances. Some patients, unlike children, find it more difficult to adapt to the separation of the bite, also experiencing pain in the area of moving teeth, masticatory muscles and temporomandibular joints. In some patients, on the contrary, with an increase in the interalveolar distance, first with an orthodontic device and then with a prosthesis, the pain from the temporomandibular joints that existed before treatment disappears.
When orthodontic treatment of various forms of progeny, one should follow a number of necessary principles and avoid making typical mistakes:
- when treating progeny using intermaxillary or extraoral traction, a necessary condition is the separation of the dentition by the amount of reverse incisal overlap;
- when treating with the piickl apparatus, it is necessary to use a chin sling with a rubber traction to the head cap, especially in the initial period of treatment, it is also necessary to grind off the unworn cusps of baby teeth;
- when using devices with an inclined plane (piickl, OM Basharova, etc.), you should not make the plane very high (7 mm or more), and also choose the correct angle of its inclination (no more than 45°);
- when using an E. Engle arch with elastic rods, you should not move all the teeth located in front of the supporting molars at once, but one by one, that is, the upper central incisors, then the lateral ones, canines, etc. As the upper teeth move in the vestibular direction using intermaxillary rubber rod, the support nuts on the upper arch should not rest against the tubes, for which they should be unscrewed when supervising the patient;
- after achieving correct incisal overlap, it is necessary to take into account the disocclusion that forms in the lateral sections, which must be eliminated to prevent overload of the anterior teeth.
The issue of tooth extraction in the treatment of progeny does not have a clear solution. Some researchers recommend removing the lower 4 teeth in case of underdevelopment of the upper jaw; others, in various forms of progeny, consider it advisable to remove 34 and 4 or 38 and 48 teeth, expressing the opinion that with the early removal of primary and permanent teeth, the basal arch of the lower jaw decreases. However, many clinicians believe that it is difficult to count on delaying the development of the body of the lower jaw when removing baby teeth and even the rudiments of permanent teeth. These formations are morphogenetically related to the alveolar process and their direct influence is limited to the development of this particular bone.
By the end of the change of primary teeth to permanent ones, therapy should be comprehensive, including orthodontic, orthopedic, and surgical measures, and the latter should play a major role. Unfortunately, there is unjustified surgical passivity in the treatment of dentofacial anomalies and deformities. As a rule, these patients undergo unsuccessful treatment with orthodontists for a long time. Later, their referral to a surgeon significantly complicates therapy.
Surgical treatment methods are clearly not used enough; questions about at what age it is more rational to perform surgical intervention, how to prevent complications and improve aesthetic results have not been resolved. A number of specialists believe that the reason for low surgical activity is the danger of relapse and numerous factors contributing to this, namely: disturbance of muscular balance due to the new, constructive position of the lower jaw, early removal of intermaxillary immobilization, insufficient preoperative preparation, and irrational postoperative period.
According to many researchers, when deciding on the surgical treatment of progenia, the patient’s complaints about aesthetic dissatisfaction, chewing and speech disorders are sufficient grounds for surgery. Although they write in a number of manuals that when planning an operation, functional disorders are brought to the fore and the goal of therapy is to achieve good articulation, and aesthetics is of secondary importance. In fact, over 72% of patients undergo surgery for aesthetic reasons.
More than 40 surgical methods for excessive development of the lower jaw are described in the specialized literature. Of these, the most common are osteotomies of the mandibular ramus (oblique sliding, based on the principle of sagittal splitting). These types of osteotomy are characterized by a wide contact surface of bone fragments and, as a result, faster consolidation, preservation of the neurovascular bundle and dentition, the ability to rotate the central fragment and, if necessary, model the angle of the lower jaw. Osteotomy in the area of the angle and ramus of the mandible allows you to correct the sagittal and transversal relationships of the jaws, as well as improve the shape of the mandibular angle.
Osteotomy and osteoectomy on the body of the lower jaw are used less frequently and the number of supporters of these methods is much smaller. Surgical intervention on the body of the lower jaw within the dentition has serious disadvantages, it is technically difficult and less favorable from an aesthetic point of view. Shortening the body of the lower jaw often leads to thickening of the cheeks and the formation of a double chin, which can cause a very unfavorable shortening of the face in the sagittal direction, that is, the depth of the face. This is especially noticeable with a short ramus of the lower jaw. True, in recent years, some surgeons consider the optimal method to be a bilateral vertical osteotomy of the body of the lower jaw, anterior to the mental foramina, and in the postoperative period, using a special apparatus, using dosed compression, the middle fragment is moved until it contacts the lateral ones. First, before surgery, teeth 34 and 44 are removed, and often also 35 and 45.
Therefore, when alternative to surgical intervention on the body of the mandible, along with the analysis of dental and jaw changes, there must be a thorough preoperative aesthetic analysis that allows one to predict a satisfactory facial profile. In some cases, intervention is required on both jaws, sometimes the use of several surgical methods. Along with the distal shift of the lower jaw, some patients require additional corrective interventions on the chin. However, most patients refuse them, being satisfied with the results achieved. The exception is patients with severe changes in the facial profile.
The surgical technique for true progeny may be the method of choice, but the final success depends not only on the method and skill of the surgeon, but to a large extent on a set of preoperative and postoperative measures carried out with the participation of specialists in various fields. We do not provide a description regarding the management of patients in the hospital after surgery, since it is carried out according to the method generally accepted by surgeons.
The duration of hospital stay after surgery was 27-40 days and intermaxillary fixation was maintained for approximately the same time. After removing the latter, it is recommended to immediately use a pre-prepared chin sling with a rubber traction to the head cap, starting with weak forces and gradually increasing them during the retention period.
Orthopedic postoperative treatment of a retention-functional nature must be carried out after each operation using any of the methods. All patients, without exception, are prescribed treatment for chin sling for 6-10 months, and this should be strictly controlled, since many patients consider it unnecessary and burdensome. It is necessary to convince and warn about the possibility of relapse, even late after surgery (10 - 16 months). You can also use base plates or a temporary prosthesis with a retraction arch, the time of use of which is necessary before creating a stable occlusion and permanent prosthetics, if it was not carried out in the preoperative period.
As a result of the operation, a new occlusion is created, which in some cases has functional and aesthetic disadvantages due to some discrepancy in the dentition. In some patients, with the help of surgery it is possible to achieve orthognathic overlap of the front teeth, in others only their direct contact. Depending on the degree, the discrepancy is eliminated by grinding (if it was carried out before surgery, then a more precise correction), inlays, cast crowns, and in the presence of defects in the dentition, appropriate fixed or removable dentures.
Analyzing the literature data on the issue of surgical treatment of progenia, it can be noted that one of the criteria for the value of a particular surgical method is the relapse rate, which ranges from 14-44%. One of the reasons for the recurrence of true progeny after surgery is the supposedly enlarged tongue, for which the bed is reduced as a result of the surgical distal shift of the lower jaw. Therefore, a number of authors, for the purpose of prevention, propose to carry out partial resection of the tongue in parallel with surgery for progeny. However, this presents certain difficulties, primarily psychologically.
A more correct, apparently, point of view of many clinicians is that the tongue pushed forward, becoming flat, is often mistaken for enlarged. This is confirmed by clinical observations. 3-4 months before the upcoming planned operation, we conducted tongue training, simulating the reduced space in advance using an “internal” duplicate dentition for the lower jaw, made on the basis of calculations using diagnostic models. The teeth of such a prosthesis must contact the antagonists in the new occlusion, that is, in the one that is planned as a result of surgery. Such a prosthesis prevents the caudal (lower) position of the tongue and at the same time can be used to replace defects in the dentition and as an orthodontic device. Fixation of the prosthesis is carried out using conventional methods. After surgery, such patients achieve good results in aesthetic and functional terms.
Preoperative tongue training contributes to the normalization of its function, early adaptation to a decrease in space, that is, the formation of a new dynamic stereotype that provides optimal conditions for speech.
Correction of bite during progenia
The choice of correction methods depends on the type of pathology and the causes of its occurrence. The orthodontic appliances used stimulate the development of the upper jaw and correct the position of the teeth. DaVinci studio dentists use:
- mouthguards;
- trainers;
- plates.
These are less painful and long-lasting methods of correction. When starting treatment in adulthood, the braces system will help you achieve the desired result. Children wear them from one to one and a half years, while adults wear them for about four years.
Serious dental deformities in the absence of a desire to use braces are treated with surgical intervention in adulthood. Surgery is a financially expensive method associated with the risk of complications. Therefore, if a dentist recommends wearing orthodontic appliances, it is better to listen to the advice.
TREATMENT
Treatment of progenia is carried out by an orthodontist. For children in the process of jaw growth, myofunctional gymnastics and massage of the alveolar process of the upper jaw are used. If necessary, plastic surgery of the frenulum of the tongue is performed, and special mouthguards and devices are used according to indications. For permanent occlusion, a brace system is indicated. Speech therapy classes are conducted in conjunction with treatment. Sometimes, with excessive pathology, there is a need for surgical treatment.
Prevention
If the pathology is not congenital, the formation of a pathological bite can be avoided by taking timely measures:
- Plan your first visit to the dentist when the child is 2-3 years old;
- stop smoking and drinking alcohol (even in small doses) while planning pregnancy and while carrying a baby;
- prevent the development of bad habits: wean your baby off thumb sucking, get rid of pacifiers and bottles in a timely manner;
- From early childhood, teach to keep your posture straight, since the interconnection of all systems in the body has been proven. Slouching changes the tilt of the head, which contributes to the constant advancement of the lower jaw forward;
- Monitor the position of the child's head during sleep. The child should not get used to placing a pillow or fist under it. Excessive pressure on the jaw creates an incorrect bite. You should also avoid throwing your head back or pressing your head to your chest.
The main signs of progeny are a signal for immediate contact with the dentist. Pay special attention to your child, because it is in childhood that pathology is easy to correct.
Add a comment
Leave your comment
Clinical picture
The process of development of the anomaly can be recognized in time, and the developed pathology is difficult not to notice. Symptoms are divided into external and internal.
External:
- direction of the movable jaw forward;
- visual elongation of the oval of the face due to a change in angle;
- uncharacteristic location or obvious enlargement of the lower lip;
- violation of the proportion of the lower and upper jaws;
- pointed chin;
- smoothing the fold connecting the mouth to the chin;
- deepening of nasolabial folds;
- jaw asymmetry.
These signs may be a manifestation of a disorder, and may also be associated with individual physiological characteristics.
Internal symptoms:
- slight lisp;
- overlap of the upper dentition with the lower one;
- violation of jaw symmetry with the mouth closed;
- chronic diseases of the oral cavity (caries, plaque, etc.);
- enlarged teeth;
- violation of chewing function.
Internal signs are difficult to notice with the naked eye, but they can be identified in time during a routine dental examination.
Symptoms and diagnosis
The characteristic symptoms of progeny are
- formation of a mouth gap;
- protrusion of the lower lip and chin forward with frequent loss of the upper lip;
- large mandibular angle;
- recession of the middle third and increase in the height of the lower third of the face.
With lower macrognathia, the face often narrows, the nasolabial folds deepen and the mental folds smooth out.
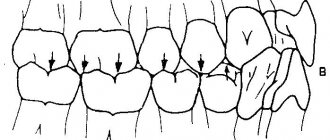
Intraoral signs of anomaly include direct occlusion of the anterior teeth and reverse incisal overlap. When the yawning teeth join together, a mesial step is formed. Diastemas, tremata, and tilting of the teeth of the lower jaw may also appear.
The sagittal relationship of the first molars is disrupted. The dimensions of the alveolar arches do not correspond to the norm, functional defects appear with a decrease in chewing efficiency.
Depending on the location, the pathology can be general or partial. General progeny is characterized by a discrepancy between the connection of the front teeth and the lateral teeth. A partial violation is characterized by a lack of closure in only one area. This may cause the jaw to shift.
Taking into account the placement and parameters of the jaw, a progenic bite is distinguished with upper micrognathia, lower macrognathia, lower prognathia, and upper retrognathia.
Diagnostic studies are carried out by an orthodontist; the research complex includes an examination of the profile and face, a visual analysis of the occlusion of the oral cavity and anthropometric data, and a functional test to distinguish false from true progeny.
Read also: 3d teeth
The level of severity of pathology is assessed based on the results of a study of diagnostic models, teleradiography, and the use of bite ridges to determine anomalies of occlusion. The doctor also performs orthopantomography, tomography and radiography.
Additionally, the patient may be sent to a speech therapist and otolaryngologist for consultation.
Preventive measures
The photo shows the patient before and after correction of progenia
According to medical data, progeny does not always manifest itself due to genetics. In order to prevent or prevent malocclusion, it is recommended to promptly treat diseases that affect the maxillofacial apparatus and regularly visit the dentist when changing primary teeth in a child.
Preventive measures include correct sleeping position, normal pregnancy and childbirth, breastfeeding, elimination of bad habits (thumb sucking, etc.).
Progenic bite is a serious orthodontic defect that can be corrected by timely contact with experienced specialists.
Possible consequences
If a person does not pay due attention to his health and does not correct a pathological progenic bite in a timely manner, then serious problems may arise. These include difficulty chewing and biting food, speech disorders and temporomandibular joint dysfunction.
Read also: When do babies start teething?
If the chewing load is incorrectly distributed in the front teeth, periodontal tissues are overloaded, and periodontal disease appears with early tooth loss. Due to improper chewing of food, gastrointestinal disorders, difficulties with swallowing and stomach irritation from rough food appear. Migraines and ringing in the ears occur. A person may experience aesthetic and emotional discomfort.
Retention period
Consolidation of the results is considered a mandatory stage of therapy. Correction of rows of teeth using hardware methods is not completed after their removal. After the main therapy, the patient goes through a retention period with the use of orthodontic structures for a long time (from six months to 2 years).
The doctor personally sets the exact period individually. To record the result, the following devices are used:
- Retainers . They are non-removable devices, shaped like a small arc made of special fiber or metal. The structure is secured from the lingual part of the teeth with a composite. They maintain the correct position of the teeth while remaining invisible.
- Trainers . Such devices are used to correct and secure the bite. Special models are used, which are worn for at least 8 hours a day. Subsequently, the duration of wear is reduced to 1-3 hours.
- Individual mouthguards made of silicone, repeating the relief of the teeth. The duration of their wear during retention is at least 20 hours a day, after which the time is reduced.