Anesthesia during dental treatment is the main achievement of modern dentistry. Without local anesthesia, only the removal of superficial caries is carried out without affecting the pulp. If the patient is terrified of medical intervention, dental procedures are performed under general anesthesia. The article will cover the question of what torus anesthesia is and in what cases it is used.
What is torusal anesthesia
Methods of pain relief during dental procedures are selected depending on the type of intervention performed and the characteristics of the clinical picture. This can be either an injection of an anesthetic into the gum (infiltration) or covering a large area of the patient’s face - conduction anesthesia. With conduction anesthesia, a bundle of nerves that transmit pain sensations to the brain is blocked.
Since there are several nerves in the oral cavity, the impact is carried out specifically on the tooth adjacent to the diseased tooth. Thus, when treating molars of the lower jaw, mandibular anesthesia is performed, a variation of which is the torus method of anesthesia. With this method of pain relief, the mandibular nerves are blocked:
- inferior alveolar;
- buccal;
- lingual.
An anesthetic solution is injected into the junction point of these nerves - the torus. As a result of infiltration of the solution, complete anesthesia of the following facial areas occurs:
- chin;
- soft tissues of the lower jaw;
- their corresponding skin.
That is, sensitivity is lost at the level of the skeletal and muscular systems, as well as the skin. The effectiveness of pain relief allows you to begin medical procedures almost immediately after instillation of the product.
The advantage of the technique is that there is a large area of the facial region that is insensitive to pain. Disadvantages are the possibility of complications after the injection and the presence of a highly qualified dentist. The doctor must have knowledge of anatomical landmarks in order to find the right point for instillation without mistakes.
Painkillers used:
- lidocaine;
- ultracaine;
- novocaine
- trimecaine.
For serious surgical interventions that require a long time, other medicinal substances with an analgesic effect are used. Trimecaine is used to remove lower molars; it effectively blocks the dental nerves. It is also used for cleaning canals and filling teeth affected by caries.
If the chewing molars remain insensitive to the action of the medicine after the injection, the dentist performs additional anesthesia: saturates the mucous membrane around the sensitive molars with the solution.
Technique of “high” anesthesia of the inferior alveolar nerve
Carrying out standard mandibular anesthesia does not always provide sufficient anesthesia of the lower jaw, which can be explained by the presence of additional innervation. The teeth of the lower jaw can receive additional innervation from the hypoglossal, auriculotemporal and upper cervical nerves. The hypoglossal branch leaves the trunk of the inferior alveolar nerve approximately 1 cm above the mandibular foramen and therefore cannot be switched off using conventional techniques. Branches from the auriculotemporal nerve extend to the pulp of the lower teeth through openings in the ramus of the lower jaw. This innervation is blocked by “high” anesthesia according to GAGow-Gates and JOAkinosi.
When to use
The effectiveness and simplicity of torusal anesthesia allows it to be used in many cases of dental practice.
Torusal anesthesia is used for:
- opening of ulcers and abscesses in the lower jaw;
- extraction of mandibular molars;
- depulpation and other methods of intervention;
- installation of fixing splints in case of injury to the mandibular region;
- removal of molars with abnormal root locations;
- surgery for broken jaw bones;
- elimination of neoplasms;
- augmentation/removal of the jawbone.
Pain relief is also carried out in case of abnormal eruption of wisdom teeth, which is accompanied by severe swelling and pain. Incorrect growth of a wisdom tooth can cause rupture of gum tissue and cause severe complications.
The effectiveness of instillation depends on the qualifications of the dentist. To simultaneously block three nerves, you need to accurately hit the point of their connection, which is located in the torus. If the doctor cannot correctly determine the location of the torus, then it will not be possible to numb the desired area of the lower part of the face.
Incomplete pain relief can lead to discomfort during dental procedures. If the patient feels that there is insufficient blockage of the facial nerves, he should immediately inform the dentist.
Anesthetics used in this method may cause allergic reactions. Therefore, you need to warn your dentist about intolerance to certain medicinal components.
Allergic reactions to drugs are another problem with anesthesia. Since quite a large number of patients are intolerant to certain substances, pain relief can cause an unpredictable reaction in the body.
Features of pain relief for temporary teeth
Of course, the choice of pain relief method depends on the planned intervention.
In the treatment of caries and pulpitis of temporary teeth, preference is given to infiltration methods carried out from the vestibular (buccal/labial) side, and there is no need for lingual or palatal anesthesia. This is explained by the predominance of spongy substance and a large number of nutrient openings in the structure of the jaw bones, facilitating the diffusion of local anesthetic.
In order to reduce the degree of pain of the injection and increase the level of comfort for the child, the following recommendations for local anesthesia should be followed:
- A preliminary distracting preparatory conversation with the child is necessary, during which the doctor uses terms that the child understands. In this case, the words “injection”, “syringe”, “anesthesia”, “removal”, “needle” are not pronounced.
- The child should not see (look at) the injection equipment. All instruments are presented by an assistant out of sight of the child.
- Application anesthesia should be performed so that the child does not feel the puncture stage of the mucous membrane.
- The rule must be observed: “one needle, one injection.” If the needle accidentally comes into contact with the bone tissue of the jaw, its tip is deformed; as a rule, it bends in the direction opposite to the bevel. A repeated injection with the same “dull” needle in another segment will involve applying pressure that is unpleasant for the child.
- The anesthetic should be injected slowly, 1 ml/min. Forced administration of the anesthetic leads to hydrodynamic tissue trauma, which causes pain.
- Two-stage injection of a portion of anesthetic. When performing infiltration anesthesia, the doctor initially injects a small amount of anesthetic? 0.1 submucosally, while a zone of tissue infiltration the size of a millet grain is visually determined. Next, the doctor talks with the child for 2-3 minutes.
- The subsequent administration of the main portion of the anesthetic is painless.
- The temperature of the anesthetic solution should be close to the child’s body temperature. To do this, do not store anesthetic carpules in the refrigerator. Before the injection, the doctor can “warm” the carpule in his hand or in running hot water.
The volume of injected anesthetic for infiltration anesthesia of temporary incisors and canines is on average 0.3 ml; for anesthesia of temporary molars, 0.5-0.6 ml is used. Subperiosteal anesthesia should not be performed as this will cause pain to the child and will not increase effectiveness. The needle should move submucosally towards the apexes of the roots of the teeth. In the upper jaw, when performing infiltration anesthesia, one should not insert a needle into the area of the frenulum of the upper lip, mucous strands in the area of temporary canines. These areas have an extensive network of nerves, providing hypersensitivity in these areas.
When performing an operation to remove temporary teeth of the upper jaw with a diagnosis of periodontitis, various combinations of infiltration methods are used. In the upper jaw, when removing incisors and canines, infiltration vestibular (0.5 ml) and incisal anesthesia (less than 0.2 ml) is used. In this case, classical conduction anesthesia with the advancement of the needle into the incisive canal is not carried out, but a certain amount of anesthetic is injected on the side of the incisive papilla, until signs of ischemia appear. If possible, painful incisal anesthesia should be avoided, which can be replaced with topical anesthesia or by inserting a needle into the vestibular interdental papilla and then moving it to the palatal side with a continuous supply of anesthetic.
The choice of dilution of the vasoconstrictor depends on the expected duration of the intervention and the presence of concomitant pathology in the child. As a rule, the duration of treatment for a child does not exceed 20-30 minutes.
When anesthetizing the first and second temporary molars, infiltration vestibular (0.5-0.6 ml) and palatal (0.2 ml) anesthesia is used. Palatal anesthesia can be replaced by the above-described approach through the interdental papilla. To reduce the degree of pain of local anesthetic injection into the hard palate, preliminary application anesthesia should be used.
When removing temporary teeth of the lower jaw with a diagnosis of periodontitis, a combination of conduction and infiltration methods is used. When removing incisors and canines, infiltration vestibular (0.3 ml) and lingual (less than 0.2 ml) anesthesia is used. Lingual infiltration anesthesia is performed in the area of the transition of the attached gum to the mobile mucosa of the floor of the mouth. The anesthetic is injected into the submucosal layer; the needle is not advanced to prevent intravascular injection. You can anesthetize the lingual mucosa by inserting a needle into the interdental papilla from the vestibular side and then moving it towards the lingual mucosa. When removing temporary first molars of the lower jaw, the above-described technique is used with the only difference that 0.5 ml of anesthetic is injected from the vestibular side of the tooth being removed. In the presence of local inflammation, it is necessary to perform conduction mental anesthesia. When removing the second temporary molars of the lower jaw with a diagnosis of periodontitis, either mandibular anesthesia (1 ml) or a combination of mental anesthesia (0.6 ml) and lingual infiltration (0.2 ml) is performed.
During the period of physiological change in occlusion, the removal of temporary teeth for orthodontic indications has some features. The most common mistake is removing a “moving” tooth under application anesthesia. The depth of application anesthesia is 2-3 mm of the mucous membrane, and the roots of the tooth may not be completely resorbed, and their removal will be painful. Application anesthesia can be used as an independent method only if the tooth is fixed by mucous membrane on one edge. In other cases, infiltration anesthesia should be performed. The anesthetic is administered before signs of gum ischemia appear; its volume is minimal.
Technique
Since the technique was developed by the Soviet dentist Weisbrem, it bears his name. In addition to Weisbrem’s technique, there are several more proven methods of torusal anesthesia developed by other experienced dentists - Legardi, Akinosi, etc.
According to Weisbrem
For the instillation of the medicine to be successful, the patient must throw back his head and open his mouth wide. During instillation, the syringe needle reaches the jawbone, so it should be held strictly perpendicular to the patient’s cheek. The success of pain relief depends on the correct location of the torus point.
The syringe needle is inserted into the soft tissues quite deeply and is located at the level of the first or second chewing molar. After inserting the needle, the medicinal composition is instilled in a volume of 1.5-2 cubes. To check that the needle has entered the blood vessel, the doctor draws a small amount of medication back into the syringe. The presence of blood in the syringe body indicates deformation of the blood vessel during instillation.
If everything went well, the doctor performs a block of the lingual nerve. No more than 0.5 ml of the medicinal composition is consumed to relieve pain. After 5 minutes, the patient should feel numbness in the mandibular region, and only after this can treatment procedures begin.
According to Akinozi
Using the technique, two nerves are blocked - the lingual and alveolar. The patient does not need to open his mouth wide; all manipulations are carried out with closed teeth. The doctor inserts the syringe needle into the point between the tubercle and the recess of the lower jaw. The volume of the drug is the same and is 1.5-2 ml. However, Akinosi anesthesia is used only in cases of ineffective blocking of nerve endings by other methods.
Despite the high effectiveness of pain relief, the method has the following risks:
- injury to the facial nerve;
- deformation of the periosteum;
- injury to the pterygoid and temporal muscles.
The Askinosi method requires a highly qualified dentist, as it is unsafe and traumatic. However, it is the Askinosie method that brings high-quality pain relief to patients who have two or more nerve endings in their molars.
According to Go-Gates
The anesthesia method was developed by Australian dentist Gou-Gates. It differs in that instillation is carried out in the corner of the patient’s lips. The syringe is inserted into the tendon of the pterygoid and temporal muscles and touches the jaw bone. After taking an aspiration sample (checking for the presence of blood in the solution), the dentist administers the medicinal composition in a volume of 1.5 -2 ml. Next, the patient should remain with his mouth open until the nerve endings are completely blocked. This takes no more than five minutes, although it is inconvenient.
Despite the inconvenience, using the Go-Gates method, several nerve roots are blocked at once:
- maxillohyoid;
- reed;
- temporal;
- buccal;
- lower lunula.
Complete blocking of the nerve roots occurs somewhat later than with other methods.
Improper instillation can cause spasm of the respiratory tract and hematoma formation. The method is one of the safest.
Local anesthesia in dentistry
In dentistry, the following types of local anesthesia are distinguished:
- Appliqué
- Infiltration
- Conductor
- Intraosseous
- Intraligamentary (intraligamentous)
- Stem
- Combined.
- Computer
All modern methods of pain relief in dentistry have their own characteristics, indications and contraindications.
In pediatric dentistry, the same types of local anesthesia are used, but for very young patients (2-3 years old), who simply will not allow the dentist to work, we give short-term anesthesia, for example, with propofol. This is a very modern and safe drug.
Application anesthesia
Allows you to anesthetize superficial soft tissues: skin and mucous membranes to a depth of approximately 1 - 3 mm. The drug quickly penetrates the tissue and temporarily disables the nerve endings located there. During the procedure, a high concentration of local anesthetic is used in the form of a gel, aerosol or emulsion. The drug is applied to the dried mucous membrane or the solution is sprayed onto it using a spray bottle.
Local topical anesthesia in dentistry (in other words, anesthesia without an injection) is used:
- to numb the needle point before injecting;
- for removing baby teeth;
- when removing small soft tissue tumors.
Pain relief for stomatitis in children using special pastes and gels is also an application.
Infiltration of tissues with anesthetic solution
Infiltration is used in dentistry much more often than other types. Tissue anesthesia occurs using a syringe or needleless injector. Sensitivity to pain is switched off after just a few minutes, and the duration of exposure depends on the type of anesthetic, its dose, and the presence of vasoconstrictor components in the composition.
The method, in addition, has some variations: intraosseous and intraligamentary anesthesia, they are also quite often used in dentistry. For them you need to use a special syringe.
Conductive anesthesia in dentistry
Conduction dental anesthesia is used much less frequently than infiltration anesthesia. An anesthetic solution is injected near the peripheral nerve trunk, which numbs the entire area for which it is responsible. The desired effect occurs 10-15 minutes after the injection and lasts for 1-2 hours.
It is used when you need to numb a large area at once or if infiltration does not work. Unlike infiltration anesthesia, a smaller amount of anesthetic is used here, but in a higher concentration.
Torusal and mandibular anesthesia are performed on the lower jaw.
In this case, the lower alveolar and lingual nerves are switched off, so during the action of the anesthetic the patient feels numbness in the entire half of the lower jaw, lip, chin and tongue. Tuberal anesthesia in dentistry is often accompanied by the formation of a hematoma. It was this inconvenience, combined with the complexity of the technique and the high likelihood of complications, that forced dentists to abandon this type of anesthesia.
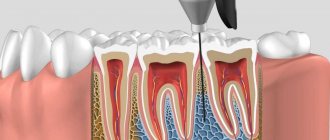
Intraosseous
To administer an anesthetic solution intraosseously during injection, the doctor perforates the dense outer cortical plate of the jaw bone and injects the solution into the spongy substance itself, where the terminal branches of the dental plexus are located. The effect appears within 1-2 minutes, the teeth and alveolar process are anesthetized. This manipulation is performed using a special syringe with a short, large-diameter needle and is a type of carpule anesthesia in dentistry.
Intraligamentary
Intraligamentary anesthesia involves the dentist injecting a solution into the periodontal ligament, which connects the tooth root to the bone alveolus. In this way, you can anesthetize only one tooth and do it with a record small amount of anesthetic, which is why this type of anesthesia remains very popular. It should be noted that the injection into the periodontium is quite painful and minor discomfort remains in the tooth for 24 hours after it is performed.
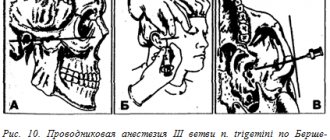
Trunk anesthesia in dentistry
This type of anesthesia is rarely performed in dentistry. This technique is also called (according to the author) “according to Bershe-Dubov”. This technique is used for severe pain in a patient, for the treatment of serious injuries and operations on the jaw and zygomatic bone, as well as for neuralgia, and only in a hospital setting.
An anesthetic injection is given at the base of the skull (brain stem), and the pain relief spreads through both trigeminal nerves and their branches. This allows you to immediately disconnect the mandibular and maxillary nerves. The effect of stem anesthesia lasts quite a long time.
Combined anesthesia
Combined or sedative anesthesia in dentistry is used more and more often. In order for the treatment to be not only painless, but also completely comfortable, it is not enough to simply eliminate pain, it is necessary to cope with fear and emotional stress. It is this effect that potentiated analgesia can achieve. It is a combination of superficial sedation and local anesthesia, carried out with the participation of an anesthesiologist. This is one of the best types of anesthesia for children in dentistry at the moment.
Superficial sedation is a state of stunning, slight depression of consciousness. In this case, the patient does not experience fear or anxiety before the upcoming intervention, but remains conscious. Of course, the advantage of this pain relief is not only its comfort. Anxiety and fear, among other things, cause a significant decrease in the pain threshold. That is, eliminating negative emotions allows you to achieve a good level of pain relief with smaller doses of anesthetic.
What is computer anesthesia?
Computer-controlled anesthesia is carried out by a special electronic system, which consists of a system unit and a handpiece. The needle has a special design that allows you to pierce soft tissue and perforate the cortical plate of the bone absolutely painlessly. Another advantage is the dosed administration of an anesthetic drug: the amount and speed of this process is controlled by a computer.
Carpule anesthesia
To perform carpule anesthesia in dentistry, special instruments are used - carpule syringes. They are a reusable metal device that has a body, a plunger and a needle that is much thinner than a regular injection needle. The drugs are supplied in special carpules and placed in the syringe body.
Danger and risks
Pain-relieving procedures require highly qualified dentists and a certain amount of caution when performing them. Improper administration of torus anesthesia can lead to the following complications:
- fracture of a syringe needle followed by surgery;
- injury to blood vessels with subsequent bleeding and hematomas;
- paralysis of facial muscles, partial loss of facial mobility;
- injury to the fibers of the pterygoid muscles;
- loss of sensitivity of the oral mucosa;
- ischemia of the chin due to penetration of the drug into the bloodstream;
- infection of tissues with subsequent development of inflammation;
- neuritis of the mandibular nerves.
However, the patient must be careful after the dentist’s manipulations:
- sanitize the oral cavity in a timely manner;
- exclude rough foods until the mucous membranes are completely healed;
- take care of liver restoration.
Any anesthesia negatively affects the health of the liver, so the patient is obliged to independently take care of his own health and take prescribed medications or use other methods of restorative procedures.
Anesthetics with low vasoconstrictor dilution 1:200000
Indicated for most outpatient interventions in pediatric dentistry. 4% articaine 1:200000 provides anesthesia for soft tissues for 180 minutes and dental pulp for 45 minutes, which satisfies the protocol for most outpatient interventions.
Currently, anesthetics based on 4% articaine with epinephrine 1:400000 have appeared in European countries. They provide anesthesia for dental pulp tissue for 20 minutes and soft tissue for 1 hour. This anesthetic provides the duration of anesthesia required by the doctor and a short period of “numb” tissue, which is so important for pediatric patients. Currently, these anesthetics are not certified in the Russian Federation, but work is underway to introduce them into domestic dentistry.
It is also worth noting that there is no difference in the depth of anesthesia and effectiveness between anesthetics with vasoconstrictors 1:100000, 1:200000 and 1:400000. There is a difference only in the duration of local anesthesia of the dental pulp: 25, 45 and 75 minutes, respectively. Many dentists mistakenly divide anesthetics into “strong” (1:100,000) and “weak” (1:200,000). This statement is misleading.
For short-term interventions in children with concomitant pathologies, the use of anesthetics without a vasoconstrictor is indicated. However, their use does not guarantee complete safety and does not reduce the risk of complications. It is worth noting some of their pharmacological features. Vasoconstrictors are added to the local anesthetic solution not only to increase the duration of pain relief, but also to reduce their toxicity. The fact is that all anesthetics have a vasodilating effect and undergo fairly rapid absorption into the bloodstream. The addition of a vasoconstrictor slows the absorption of the anesthetic and prolongs its action. When using an anesthetic without vasoconstrictors, this effect does not occur. The anesthetic is forced into the blood, which can lead to a toxic reaction. This complication is possible if the permissible dosage is exceeded, which is different for anesthetics with and without a vasoconstrictor. In summary, it should be noted that anesthetics without a vasoconstrictor do not affect the functioning of the cardiovascular system, are less allergenic since they do not contain preservatives, but due to accelerated absorption they are toxic and safe to use only if the dosage is observed.
Contraindications for carrying out
In what cases is local anesthesia of the oral cavity contraindicated or has partial contraindications? Anesthesia is prohibited for any liver pathologies, as it directly affects liver cells. Due to the high dose of novocaine, this method is excluded from the permissible method, and general anesthesia is recommended instead.
Also, torusal anesthesia is contraindicated for:
- intolerance to the components of the medicinal substance;
- pathologies of the circulatory system;
- mental disorders;
- bronchial asthma;
- cardiovascular pathologies;
- epileptic seizures.
Also, local anesthesia of this method is not carried out in case of anatomical disorders in the structure of the jaw and gums, as well as when the point of connection of the nerves is shifted.
Can this anesthesia be used during pregnancy? Permission must be given by the treating gynecologist, since the method may pose a certain danger to the fetus.
Bottom line
Torusal anesthesia is an effective means for quickly numbing a large area of the facial area. It is performed during complex dental procedures, when it is necessary to numb a large area of the facial region for a long time. With one injection, it is possible to immediately block three facial nerves that react acutely to pain.
However, performing the manipulation requires high medical qualifications, knowledge of the anatomy of the location of nerve endings, and careful handling of instruments. Improper administration of a drug can lead to various complications and injure the patient. The technique is used when other methods of blocking nerve endings are ineffective.
Sources used:
- Basic methods of pain relief at an outpatient dental appointment / Samedov Timur Islamovich. - M.: SpetsLit, 2011.
- Local anesthesia in dentistry / E.A. Bazikyan. - M.: GEOTAR-Media, 2012.
- Therapeutic dentistry. Anesthesia. Bleaching. Filling. Endodontics / Edited by E.V. Borovsky. - M.: Dentistry, 2005.