3D diagnostics and principles of visualization of 3 molars of the lower jaw
Rogatskin D. V. Radiologist, Ortos LLC (Smolensk)
A fragment of a chapter from the forthcoming book “Radiodiagnosis in Dentistry. 2D/3D".
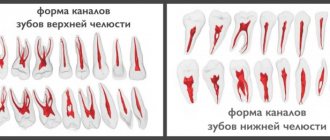
Teeth 48, 38, often called “lower wisdom teeth,” usually have a two- or three-root structure, but the length and configuration of the roots are extremely variable. These can be either short fused roots or excessively long curved ones with pronounced divergence (Fig. 1).
Rice. 1. Fragment of a panoramic tomogram, the area of the molars of the lower jaw on the left. The anterior root of tooth 38 is enlarged and curved. The shadow of the root crosses the lumen of the mandibular canal.
There are a number of clinical indications for the removal of third molars of the mandible, however, surgical intervention is often complex and complicated, so at the planning stage there is a need for careful preoperative diagnosis. This is due to the fact that these teeth occupy a distal position in the dentition and are often in a state of retention. According to modern studies, complications associated with damage to the mandibular nerve occur on average in 13% of cases of the total number of removals (Wang et. al., 2016). Traditional diagnosis of the position of the mandibular canal relative to the roots of the third molar using a panoramic image can no longer be considered sufficient and objective. In some cases, a three-dimensional study performed for clarification forces the surgeon to change the intervention tactics (Matzen et. al, 2013).
Impacted teeth are teeth that have not fully erupted due to difficult conditions for eruption, or have formed impacted, that is, completely immersed in bone tissue.
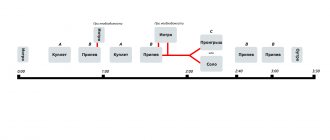
To describe the position of the third molar, we can recommend the principles laid down in the Winter and Pall-Gregory classifications. Winter (1926) assessed the position of the vertical axis of the wisdom tooth relative to the 2nd molar and identified 5 position options - vertical (V - in Fig. 2), mesial inclination (M - in Fig. 2), horizontal position (H - in Fig. 2), transversal position, distal tilt and inversion. To this it should be added that the wisdom tooth can also be in an ectopic position - that is, outside the dentition, for example, in the jaw branch. The Pell-Gregory classification (Pell&Gregory, 1933) is based on determining the degree of immersion of the 8th tooth relative to the crown of the 7th and the degree of overlap of the crown of the 8th by the bone tissue of the anterior edge of the jaw branch. The authors distinguish 3 classes of overlap (Fig. 2):
- 1 – the crown is not covered by bone tissue
- 2 – bone tissue covers up to half of the crown surface
- 3 – the crown is completely immersed vertically in the bone tissue
and 3 levels of immersion:
- A – the crown of the 3rd molar is in contact with the crown of the 2nd molar
- B - the crown of the 3rd molar is in contact with the cervical region of the 2nd molar
- C - the crown of the 3rd molar is in contact with the root of the 2nd molar
Depending on the class, level and relationship of the root with the mandibular nerve, the surgeon chooses the method of tooth fragmentation and determines the tactics of surgical intervention (Maegawa et al., 2003).
Rice. 2. Illustration for the classification of the position of the 3rd molars of the lower jaw according to Pell&Gregory, Winter. Visualization based on panoramic tomograms. Vertical columns: V – vertical position, M – mesial slope, H – horizontal position. Horizontal rows: A, B, C - immersion levels (explanation in the text). The numbers in the table cells indicate the degree of overlap of the crown with bone tissue.
In 2015, Italian researchers (Maglione et al.) proposed a detailed and rather complex classification of the relationship between the roots of impacted wisdom teeth and the mandibular nerve. The authors identified 7 classes and a number of subclasses. It is likely that the proposed gradation has important clinical significance, but from the point of view of primary diagnosis and description of the tomogram, such detail may be regarded as unnecessary. For diagnostic purposes, Chinese experts only propose to state that the nerve passes below the tooth, vestibular from the root, lingually or between the roots (Wang et. al., 2016). In this context, this approach is the simplest and most logical. However, there are a number of nuances associated with the features of the virtual positioning of the software coordinate system.
First of all, it is quite difficult to adequately assess the relationship between the root and the mandibular canal with a minimum of options and using a non-interactive coordinate system fixed in the anthropometric position. In this case, the area under study is visualized in an oblique section without taking into account the individual structure and position of the tooth; the shape, size and relationship of the structures are conveyed with distortion, and there is no information about the neighboring tooth (Fig. 3). To obtain the most informative image, it is necessary to orient the axial and sagittal planes according to the mesio-distal length of the canal, taking into account its position and configuration, and fix the coronal plane at the point of greatest contact of the root with the nerve (Fig. 4, 11). Optimal visualization is carried out in three dimensions, indicating the location through which the main section passes. The working depth of the layer for the axial and coronal sections is recommended to be minimal, for the sagittal (mesio-distal section) - a zonogram from 3 to 10 mm. In addition, for each case, standardized polypositional visualization of objects is necessary - separately the tooth, in order to assess its structure and configuration (Fig. 5), and separately the relationship of the root with the mandibular nerve if their contact is visually determined (Fig. 6). For this purpose, the following formulations can be recommended:
- I – inferior – the nerve is in a lower position relative to the tooth. Periapical (apical) in a vertical position and mesial tilt - IA (Fig. 7), periradicular in a horizontal position - IR (Fig. 6). In the case of simultaneous periradicular inferior fit and periapical distal, in a horizontal position or mesial tilt - IRD (Fig. 8).
- L – lateralis – the nerve is located on the side of the tooth. LL – lingual or LB – buccal (Fig. 4).
- IR – inter-radicularis – the nerve is located between the roots in the furcation area. In this case, there can be two options: IR1 - the apices of the roots do not close under the nerve (Fig. 9), IR2 - the apices of the roots close under the nerve, enveloping it in a ring (Fig. 10).
Rice. 3. An example of incorrect visualization of tooth 48 and its relationship with the mandibular nerve.
Rice. 4. The same tooth (Fig. 3), correct MPR visualization using an interactive coordinate system and adjustable depth of the selected layer. Targeted visualization of tooth 48 and the mandibular canal. The depth of the selected layer is 5 mm. Immersion level B, degree of crown overlap 3, position M, relationship with nerve LL – B3, M, LL (explanation in the text).
Rice. 5. Targeted imaging of tooth 46, MPR. The axial section is longitudinal along the distal (“upper”) root. A two-root structure, a pericoronal decrease in the density of bone tissue of a hemispherical shape is determined, corresponding to the initial signs of the development of an odontogenic cyst. C3, H, IRD.
Rice. 6. The same tooth (Fig. 5), transverse and longitudinal section (coronal and sagittal reformats), targeted visualization of the relationship of the root of tooth 48 with the mandibular nerve. The correct location of coordinates to determine the lower contact with the root along the length.
Rice. 7. Correct position of coordinates for the purpose of visualizing the relationship of the anterior root of tooth 48 with the mandibular nerve at B2, V, IA.
Rice. 8. Three-dimensional visualization of the lower and distal relationship of the root of tooth 48 with the mandibular nerve along its length. C3, H, IRD, length 10 mm.
Rice. 9. MPR, position of the nerve between the roots of tooth 38 without closure of the apexes. B2, M, IR1.
Fig. 10. MPR, position of the nerve between the roots of tooth 38 with closed apexes. C3, M, IR2.
The above abbreviations and designations characterizing the position of the third molars and the relationship of their roots with the mandibular canal can be used as indices in statistical studies. For example, in Fig. 4, the position of the tooth corresponds to the index B3, M, LL, where B is the level of immersion, 3 is the degree of crown overlap, M is the position of the tooth relative to the vertical axis and LL is the relationship with the nerve (see Fig. 2).
In some cases, the mandibular canal is defined as being located at some distance from the root of the impacted tooth (Fig. 11). In addition, the bone marrow space present in the lower position can simulate the lumen of the mandibular canal (Fig. 12).
Rice. 11. Transverse and longitudinal section through the mesial root of tooth 38. The root is curved in the vesibulo-oral direction, the apical part is located at a distance from the canal of the mandibular nerve.
Rice. 12. MPR. Visualization of the distal root of tooth 38. B3, M, LL. Lateral-lingual position of the nerve relative to the root, periapical decrease in bone density due to the presence of bone marrow space.
The contact of the tooth with the nerve can be either point-like or over a certain extent relative to the surface of the tooth, for example, lower and distal contact with mesial inclination and horizontal position (Fig. 5, 6, 8). In such cases, the location and extent of the intended contact should be indicated.
Thus, in the process of initial diagnosis of the condition and position of the third molars of the mandible, the following aspects should be assessed and described:
- The shape, configuration and degree of preservation of the tooth itself;
- Degree of immersion relative to the 2nd molar;
- The degree of overlap of the crown with bone tissue;
The presence or absence of an inclination of the vertical axis of the 3rd molar relative to the 2nd, the presence of inversion, transverse position or ectopia;
- Relationship between the root and the mandibular canal;
- The presence of pathological changes in the surrounding bone tissue.
Fully erupted third molars can be partially blocked by soft tissues of the retromolar region, which contributes to the development of pericoronitis - inflammation of the overhanging gingival hood, which in turn creates conditions for the formation of a paradental cyst - Craig's cyst, retromolar cyst (Fig. 13). This cyst, like a radicular one, is inflammatory, that is, it arises as a result of a chronic inflammatory process. It was described as an independent pathological condition in 1976 (Craig). It develops in the cervical region of wisdom teeth standing in the dentition or slightly immersed vertically, most often distally, but can also form from the lingual or vestibular surface (Fig. 14). In the process of its development, it destroys bone tissue in the retromolar area, easily suppurates, complicates the removal of the causative tooth, and in rare cases, spontaneous regression of the paradental cyst is observed.
Rice. 13. MPR. Paradental cyst in the retromolar region associated with tooth 38.
Rice. 14. MPR. Paradental cyst with vestibular growth associated with tooth 38.
The most common pathological condition associated with the presence of an impacted wisdom tooth is an odontogenic cyst, which is traditionally called a follicular cyst. Unlike Craig's periodontal cyst, it is not inflammatory and can develop around the crown of any impacted tooth. The definition of “follicular” is no longer used in modern classifications or is referred to as a synonym, since this term was considered incorrect (Browne & Smith, 1991). Firstly, the definition of “follicular cyst” was used in gynecology and dermatology much earlier than in dentistry. Secondly, the process does not originate from the tooth follicle itself, but from the preserved enamel epithelium of the formed tooth crown. In the English-language literature, the definition used for this pathological condition is dentigeros cyst - “dental cyst”, “cyst from the tooth”, that is, in fact, the translation of the term cysta odontogenica - odontogenic cyst.
The definition of “tooth-bearing cyst” is incorrect, since in the lumen of the cyst in this pathological condition there is only the crown of the tooth, the shell is fixed in the cervical region, and the root remains in intact bone tissue.
Radiologically, two-dimensional images usually distinguish between central, lateral and circumferential types of growth of dental cysts (Shear & Speight, 2007). In the central type, the clearing evenly surrounds the crown along the perimeter; in the lateral type, the lumen of the cyst extends to one side of the crown—mesially or distally. With the circumferential type of growth, the shadow of the tooth is completely projected onto the lumen of the cyst, creating the impression that it “envelops” most of the root. However, this effect should rather be considered as a two-dimensional projection summation of the cyst lumen and the shadow of the tooth. When working with a three-dimensional image, the determination of the central (Fig. 15) and lateral type of growth of the odontogenic whale remains relevant. In the lateral type, mesial growth is usually observed from teeth with a mesial inclination or a horizontal position of the tooth axis (Fig. 16) and the caudal body of the mandible itself is subject to destruction. Such cysts quite quickly cause symptoms associated with compression of the mandibular nerve or suppuration. With the distal type of growth, the angle and branch of the jaw are destroyed (Fig. 17). Such cysts are rare, can reach large sizes and do not cause any symptoms for a long time. In both cases, the crown is defined as being completely located in the lumen of destruction, and the root as being located mostly in the bone tissue.
Rice. 15. MPR. Odontogenic (follicular) cyst from tooth 48 with a central type of growth.
Rice. 16. MPR. Odontogenic cyst from tooth 38 with a lateral mesial type of growth.
Rice. 17. MPR. Odontogenic cyst from tooth 38 with a lateral distal type of growth.
Simple odontogenic cysts should be differentiated from tooth-related odontogenic keratocysts (Fig. 18), inflammatory paradental cysts (Fig. 13, 14), intraluminal (unicistic, single-chamber) ameloblastomas (Fig. 19) and odontogenic ameloblastic fibromas (Fig. 20).
Rice. 18. Panoramic reformat. Keratocyst associated with tooth 48.
Rice. 19. MPR. Intraluminal ameloblastoma associated with tooth 37.
Rice. 20. MPR. Ameloblastic fibroma associated with tooth 37.
The lower third molars sometimes develop abnormally. The most common anomaly in the development of wisdom teeth is radicular dilaceration - curvature of the root at a large angle (Fig. 1, 21) and the presence of an additional lingual root (Fig. 22). In addition, the third molars themselves can be formed as a simple or compound odontoma (Fig. 23).
Rice. 21. Sagittal reformat mesio-distal section of the area of teeth 37, 38. Dilaceration of the root of tooth 38.
Rice. 22. MPR. Focused visualization of the additional lingual root (radix entomolaris) of tooth 38. The root is curved at a right angle relative to the axis of the tooth.
Rice. 23. MPR. Composite odontoma developed instead of tooth 48, impaction of tooth 37, 4-root structure of tooth 37, position of the mandibular nerve between the roots of tooth 37.
Information about the author/literature Dmitry Vasilievich Rogatskin, radiologist at Ortos LLC, Russia, Smolensk
Rogatskin DV, radiologist, LLC Ortos, Russia, Smolensk
3D diagnostics and visualization principles of 3 molars of the lower jaw
Annotation. According to modern research, complications associated with damage to the mandibular nerve occur on average in 13% of cases of the total number of removals. Traditional diagnosis of the position of the mandibular canal relative to the roots of the third molar using a panoramic image can no longer be considered sufficient and objective. In this article, which is an excerpt from the book “Radiodiagnosis in Dentistry. 2D/3D”, describes the principles and methods of visualization of the 3rd molars of the lower jaw. The descriptions are supplemented with detailed illustrations from medical practice.
Annotation. According to modern research, complications associated with damage to the mandibular nerve occur on average in 13% of the total number of removals. The traditional diagnosis of the position of the mandibular canal relative to the roots of the third molar using a panoramic image can no longer be considered sufficient and objective. In this article, which is a fragment from the book “Radio Diagnostics in Dentistry. 2D / 3D ”, describes the principles and methods of visualization of 3 molars of the lower jaw. Descriptions are supplemented by detailed illustrations from medical practice.
Key words: lower wisdom teeth; damage to the mandibular nerve; impacted teeth; follicular cyst; three-dimensional images.
Key words: lower teeth of wisdom; damage to the mandibular nerve; retarded teeth; follicular cyst; three-dimensional images.
Literature
- Maglione M, Costantinides F, Bazzocchi G. Classification of impacted mandibular third molars on cone-beam CT images. J Clin Exp Dent. 2015;7(2):e224-31.
- Winter GB Impacted mandibular third molars. St. Louis: American Medical Book Co.; 1926. p. 241–79.
- Pell GJ, Gregory BT. Impacted mandibular third molars: classification and modified techniques for removal. Dent Digest 1933;39:330–338.
- Dongmiao Wang, Tangyi Lin, Yanling Wang, Chao Sun, Lianfeng Yang, Hongbing Jiang, Jie Cheng. Radiographic features of anatomic relationship between impacted third molar and inferior alveolar canal on coronal CBCT images: risk factors for nerve injury after tooth extraction. Arch Med Sci. 2022 Apr;14(3):532-540.
- Matzen LH, Christensen J, Hintze H, Schou S, Wenzel A. Influence of cone beam CT on treatment plan before surgical intervention of mandibular third molars and impact of radiographic factors on deciding on coronectomy vs surgical removal. Dentomaxillofac Radiol. 2013;42(1):98870341.Epub 2012 Aug 29.
- Hidenobu Maegawa, Kazuo Sano, Yoshimasa Kitagawa, Toshiyuki Ogasawara, Kazuki Miyauchi, Joji Sekine, Tsugio Inokuchi, Preoperative assessment of the relationship between the mandibular third molar and the mandibular canal by axial computed tomography with coronal and sagittal reconstruction Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:639-46
- Craig G.T. The paradental cyst. A specifi c infl ammatory odontogenic cyst. Br Dent J 1976;141:9-14.
- Browne RM, Smith AJ. Pathogenesis of odontogenic cysts. In: Browne RM, editor. Investigative Pathology of the Odontogenic Cyst. Boca Ratonl: CRC Press; 1991. pp. 88–10
- Shear M, Speight P: Cysts of the oral and maxillofacial regions, ed 4, Oxford, 2007, Blackwell.