In the lateral sections, teeth (molars, premolars) are subject to regular high loads, while their anatomical structure and location in the dentition makes care more difficult. Therefore, chewing units are destroyed faster due to various injuries and dental diseases. Prosthetics of molars and premolars involves the use of structures made of durable, reliable materials that are resistant to severe chewing loads. Dental crowns are orthopedic structures for single restorations, indicated when the upper part of the tooth is destroyed by more than 60%, when the installation of a filling is ineffective.
Types of dental crowns for chewing teeth
Molars and premolars are a kind of millstones that grind food before it enters the esophagus. They experience a high load, which can exceed 75 kg per 1 cm2. Therefore, chewing units are characterized by a massive size, a surface with many protruding tubercles. To restore molars and premolars, strong, reliable materials are used that can withstand increased loads. Orthopedic dentistry offers the following types of crowns for chewing teeth:
- Metal
– durable, corrosion-resistant, service life up to 10-12 years. The list of materials from which these structures are created includes: nickel-chromium alloy, cobalt-chromium alloy, titanium, alloys of noble metals (platinum, silver, gold, palladium). Solid metal alloy prostheses can be coated or not. These are the most inexpensive crowns, but the aesthetics leave much to be desired. Structures containing gold are characterized by high ductility and fit precisely to the tooth stump. The disadvantages of such dentures include excessive abrasion of the antagonist tooth (molar, premolar on the opposite jaw) with constant contact, poor aesthetics, and the development of allergies to the components of the metal alloy (beryllium, chromium, nickel). - Metal-ceramic
- reliable, durable dentures with a metal frame coated with a layer of ceramic mass. Metal-ceramic crowns are quite aesthetic, with an optimal ratio of reasonable price and good quality. Over time, the metal base begins to appear through the gums (gray stripe effect), which negatively affects the aesthetics. Therefore, it is not recommended to place such dentures on teeth along the smile line. - Crowns made of zirconium dioxide
are strong, durable structures that retain their original appearance throughout their service life (more than 15 years). The aesthetics are not inferior to ceramics and provide the tooth with a natural appearance. The biocompatible material is suitable for patients with metal allergies and is used for restoration of the frontal and chewing areas. The structures are manufactured using CAD/CAM technology, on a robotic machine, by milling. This eliminates any errors or inaccuracies, ensures precise fit of the structure to the tooth stump and gum, taking into account the type of jaw closure and the characteristics of the bite. - Metal-plastic
- inexpensive structures, which are a frame made of a metal alloy lined with plastic mass. Due to the porosity of the material, the surface of the prosthesis quickly darkens and absorbs dyes and odors from foods, drinks, and cigarettes. The metal alloy can provoke inflammation and allergies. Service life up to 3 years. Typically, such products are used for temporary prosthetics; they are unreliable as a permanent prosthetic structure.
Ceramic crowns are not suitable for the restoration of molars and premolars. Fragile ceramics are not able to withstand high chewing loads and quickly chip and crack. Ceramic crowns are placed on the front teeth, where the main criterion is high aesthetics. The incisors and canines are not subject to high loads, but participate in the formation of a smile and are visible during conversation. Ceramic restorations are identical to natural enamel in color and transparency and do not stand out from the dentition.
Tooth anatomy
The structure of a tooth has three functional parts: crown, neck, and root.
The crown is the part of the tooth that protrudes from the gums and performs the main functions of the tooth. The root holds the tooth in the jaw, the neck is the area of the tooth between the root and the crown.
The outside of the crown is covered with a layer of fluorapatite enamel, which protects the main layer of the tooth - dentin. Dentin consists of hydroxyapatite, impregnated with calcium salts, penetrated by dentinal tubules and collagen fibers. Inside the tooth there is pulp - soft tissue with nerve fibers and capillaries.
The surface layer of the tooth root, cement, differs in chemical composition and physical properties from both enamel and dentin. The number of roots of different types of teeth is different, normally 1-3. The roots of the teeth are surrounded by elastic ligaments - periodontal tissue, which hold the tooth in the alveolus. The alveolar wall, ligaments and dental cement form the periodontium.
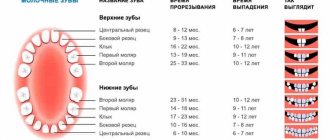
The temporary (baby) set consists of 20 teeth. During the change of teeth, not only the replacement of baby teeth with permanent teeth occurs, but also the eruption of missing teeth. A complete set of an adult contains 32 teeth: incisors, canines, premolars (small molars), molars (large molars).
Stages of installing a crown on a chewing tooth
- Diagnostics
– a comprehensive examination (orthopantomogram, 3D tomography), the dentist determines the general condition of the oral cavity, identifies dental problems, the presence of contraindications, draws up a treatment plan, and selects the optimal orthopedic design. - Preparation
- sanitization of the mouth (removal of plaque, tartar), treatment of teeth and gums (according to indications). The tooth is prepared for covering with a crown - the enamel is prepared, giving the stump the desired shape, the nerve is removed, the canals are filled, and, if necessary, the root is strengthened with a pin or inlay. To install zirconium structures, minimal tissue grinding is required; at the ILATAN clinic, a dental microscope is used for preparation, which allows you to remove enamel within a fraction of a millimeter. - Casts
- the doctor takes impressions of the patient’s jaws, from which a prosthesis is made in the laboratory. To protect the tissue, a temporary plastic crown is fixed to the prepared tooth. - Installation
- the finished crown is tried on, adjusted if necessary and fixed to the support with dental cement.
When are crowns used?
To restore an extracted or damaged tooth that bears a large functional load, a crown is used. This denture is a miniature cap-shaped dental structure that is shaped like the tooth it is replacing. The onlay completely covers the part of the tooth located above the gum.
The best crowns for chewing teeth
Since the main requirements for prosthetics of molars and premolars are the strength and durability of orthopedic systems, the best crowns for chewing teeth are made of zirconium or metal-ceramics. Zirconium is the most durable, lightweight material; installation of such structures requires minimal preparation of the abutment tooth, which is a big advantage over metal-ceramic products. The doctor will decide which restoration to use in a particular case after a detailed assessment of the clinical picture, the characteristics of the patient’s body, his wishes and financial capabilities.
How much do crowns cost in Moscow?
The cost of treatment depends on the complexity of the case, the volume of intervention, restoration material, and manufacturing technology. Installation of metal crowns in Moscow costs on average from 10,000 rubles. per unit, metal ceramics will cost from 15,000 rubles, and a zirconium dioxide crown – from 30,000 rubles.
The ILATAN clinic operates a case payment system, which protects the patient from unexpected expenses and hidden fees. The turnkey price includes all necessary measures for tooth restoration - from consultation to manufacturing and installation of a crown. Treatment of teeth, gums, production and installation of a core inlay, dismantling of old restorations are paid separately. The doctor will announce the exact amount of treatment during the consultation, after examination and diagnosis.
Fangs
The third teeth in a row from the center of the dentition. They have one long root and are distinguished by large chisel-shaped crowns. The physiological role of fangs is to bite and tear food. These teeth are the most resistant to various damages.
Physiologically, a complete set of adult permanent teeth consists of 32 teeth - 8 incisors, 4 canines, 8 premolars (small molars) and 12 molars (large molars). Their combination on the upper and lower jaws makes up the dentition.
Filling as part of caries treatment
The cause of molar destruction is most often caries, which usually develops due to abundant accumulations of plaque and hard deposits - the result of insufficient cleaning and hygiene. As a result, the tooth gradually deteriorates, and before the infection reaches the nerve, it is important to begin treatment as soon as possible. At the appointment, the dentist will remove all necrotic and damaged tissue, perform an antiseptic treatment and begin restoring the integrity of the crown.
Source: dentalperfection.in
Today, modern photopolymer materials are used for this purpose - such composites harden under the influence of a special polymerizing lamp. This property allows you to apply the material in layers to return the crown to its original appearance - it helps to recreate the anatomical relief as accurately as possible to restore the aesthetics and functionality of the tooth. In addition, photopolymers are durable and wear-resistant - their service life can reach 20 years, of course, with proper and regular care.
Dental formula
To understand how to count teeth, you can use a dental formula. It indicates the arrangement of elements in order, which is written using specialized notations. This is how the formula with the numbering of teeth is determined. The doctor examines the jaw and draws it up. The radical units are designated by Arabic values, and the temporal ones by Roman ones. The symbol looks like this:
I2/2C1/1P2/2M3/3=32.
In the expression, incisors are designated – I, premolars – P, molars – M.
In addition, dentists use tooth numbering. It is counted from the middle of the segment in the direction from left to right. Sometimes a number is added to the ordinal value to indicate the location zone. For example, the right canine on the top row is numbered thirteen.
ALTERNATIVE METHODS
In the absence of lateral chewing teeth, only removable prosthetics can be considered as an alternative technique. It is often not possible to install a bridge. To fasten it, two teeth are needed - and the end defect of the row is characterized by the presence of support on only one side. That is why the only solution is a removable denture fixed to the gums and partially preserved teeth.
A removable denture is a fairly inexpensive design that is accessible to a large number of patients from a financial point of view. But if we consider its effectiveness, we can highlight quite a few negative aspects of wearing it:
- discomfort - the prosthesis has a fairly massive acrylic gum, so it can rub and put pressure on the gums, especially during the period of adaptation,
- quite poor fixation - often patients need to use additional means (glue, ointment, gel),
- no load on the bone - it sags and atrophies because it does not receive pressure, so over time the prosthesis will be attached unevenly, and frequent relining will be necessary.
If you choose between a removable denture and a denture fixed on implants to restore chewing teeth, the second option is more preferable. In terms of comfort, durability, functionality and normalization of the entire jaw system.
1 According to the World Health Organization (WHO). 2 According to wikipedia.org.
Zsigmondy-Palmer system
It was developed independently by two dentists. In 1861, it was first introduced by the Hungarian physician Adolf Zsigmondy. In 1970, independently of Zsigmondy, a similar system was introduced by Ohio dentist Gordon Palmer. Therefore, in the USA it is better known as the “Palmer system”. In international practice, this method of numbering teeth is known as the Zsigmondy Palmer system.
The teeth located in each quadrant of the jaw received their numbers from 1 to 8. The central incisor is number 1, the third molar is 8. The numbering of the teeth in each segment is the same, and their location is indicated by graphic signs in the shape of a corner. In the corner, a vertical line denotes a conditional axis that passes through the middle part of the face. The horizontal divides the jaws. Each segment of the jaw received its own sign. To indicate whether a tooth is on the right or left, the dentist simply draws a corner on the desired side of the number.
To designate permanent teeth, Zsigmondy introduced numbers from 1 to 8, written in Arabic numerals. Since children have 20 primary teeth, 5 in each segment, they are designated by Roman numerals from I to V. In Palmer’s system, not numbers were used to designate primary teeth, but Latin letters from A to E. Therefore, both of these can still be found designations.
One of the advantages of the Zsigmondy-Palmer classification is its clarity and simplicity. In the dental chart, you can immediately see which tooth we are talking about. But it has one drawback. Using this classification method in oral communication is very difficult. Nowadays, due to its clarity, this numbering method is widely used in maxillofacial surgery and orthopedics.
Numbering for an abnormal number of teeth
If a person has a normal number of teeth in his mouth, then their numbering does not cause difficulties and remains constant both at a young age and after 60 years.
If some teeth are lost (for example, due to various diseases or developmental anomalies), then in the dental formula next to the corresponding number its absence is simply indicated.
But there are diseases of the dental system, which are characterized by an increase in the number of teeth with an atypical arrangement. With such options, the use of any numbering schemes is difficult and most often dentists refuse to use them. In this case, complete information about the number of teeth, their description and location is entered into the patient’s medical documentation.
Universal system
It was developed in 1882 by Jesus Perreidt. To this day, this numbering method remains the simplest. Each tooth has its own specific number. The American Dental Association (ADA) approved this system in 1975. Since then, it has been a staple in US dental clinics.
Number 1 in the ADA system was given to the upper right molar. The remaining teeth are numbered clockwise from it. The lower right molar has the number 32. There are two designations for primary teeth - in Latin letters from A to T or numbers from 1 to 20 with the letter d.
Despite the apparent simplicity of the ADA system, it has a significant drawback. The number does not correlate with any anatomical features, so they need to be remembered. An advantage of the method is the convenience of notation on computer models.
Why do you need to build bone tissue?
Increasing bone volume (osteoplasty) is necessary for the primary stabilization of the titanium root. If the height and width of the alveolar ridge are insufficient, the implant simply will not stay in the bone. The method of osteoplastic intervention depends on the clinical picture.
The following methods are used to build bone in the lower jaw:
- Guided bone regeneration.
Increasing the height and width of the alveolar process by replanting osteoplastic material. The surgeon peels off the gum, fills the jaw bone with osteoplastic material, closes it with a barrier membrane and applies sutures. - Splitting of the alveolar process.
Increases bone width. The doctor makes a cut in the center of the ridge, alternately screws spreaders of different diameters into it (from smaller to larger), and fills the resulting space with bone granules. - Bone block transplantation.
An autogenous (taken from the patient) bone block is screwed to the bone, covered with a collagen membrane and sutured. The 6th tooth implant is installed after the block has healed. - Increasing the volume of the maxillary bone.
Because the maxillary structures are located close to the root system of the first molars, a sinus lift is required in 90% of cases. It can be closed or open. The essence of the operation is that the doctor carefully lifts the lower part of the maxillary sinus, fills the resulting space with osteoplastic material and installs a six implant.