What you will learn in this article:
- What is this anyway? Root caries, definition.
- Its prevalence and relevance of this problem. Epidemiology of root caries.
- What is it like? Classification of root caries.
- What causes this problem? The mechanism of development of tooth root caries.
- How to find this disease in a patient? Diagnosis of root caries.
- What will we see in the mouth? Clinical manifestations of root caries.
- How is this treated? Tooth root caries treatment.
Ready? Then let's get started!
Epidemiology of root caries
The incidence of root caries is constantly increasing in older people. This is due to the fact that:
- There are more people with periodontal diseases, since their prevention is ineffective
- Dental care has improved, and retirees now have many more teeth in their mouths.
- Well, life expectancy has increased, where would we be without it?
Be that as it may, in our country today people suffer from root caries
- 1.3% aged 25-29 years
- and 35.2% (aged 55-64 years)
Contraindications
Caries is a disease that has no absolute contraindications to treatment. But if certain factors are present, treatment may be delayed or interrupted until they are eliminated. These factors include: the presence of intolerance to drugs and materials that are planned for use in treatment; concomitant diseases aggravating treatment; inadequate psycho-emotional state of the patient before treatment; acute lesions of the oral mucosa and red border of the lips; acute inflammatory diseases of organs and tissues of the mouth; a life-threatening acute condition/disease or exacerbation of a chronic disease (including myocardial infarction, acute cerebrovascular accident), which developed less than 6 months before seeking this dental care; periodontal tissue diseases in the acute stage; unsatisfactory hygienic condition of the oral cavity.
Classification of root caries
In the International Classification of Diseases (ICD-10), root caries is located in section K02 dental caries. This is the classification:
K02 Dental caries
- K02.0 Enamel caries
- K02.1 Dentin caries – here too
- K02.2 Cement caries - here it is
- K02.3 Suspended dental caries – here too
- K02.4 Odontoclasia
- K02.8 Other specified dental caries
- K02.9 Dental caries, unspecified
Classification of root caries according to Leus
Leus P.A. , Borisenko L.G.
According to the depth of damage to root tissue:
- No cavity formation
- With the formation of a cavity
According to the course of root caries:
- Active lesion
- Suspended caries
- Secondary caries (active or inactive)
- Unspecified
Modern systems for assessing and recording dental caries. literature review
Dental caries is a disease of the hard tissues of teeth, caused mainly by an imbalance between the processes of demineralization and remineralization. This disease is the leading cause of tooth loss and toothache worldwide. However, many developed countries are characterized by a decrease in the incidence of dental caries due to the active use of fluorides, improved dental care for the population and the implementation of effective prevention programs [35].
The living conditions of modern humans are caused by environmental pollution, especially in areas of environmental risk with a complex climatic and geographical location, which include the Arkhangelsk Region (AO) [11, 12, 17]. The results of various studies conducted both on the territory of the Autonomous Okrug and in other regions of the Far North with a difficult environmental situation have established the influence of environmental and hygienic factors on dental morbidity in both children and adults in Russia [1, 3, 4, 6, 7, 10, 15–17]. In connection with government programs for the development of the Arctic, measures to protect public health are becoming important. Of particular relevance is the study of cariogenic risk in pediatric dentistry, since any concentrations and doses of harmful substances are dangerous for actively growing tissues of the maxillofacial area, and the younger the child is, the more sensitive his body is to pathogenic environmental factors [8]. The study of dental caries from the point of view of medical geography is dictated by the need to obtain information about the prevalence and intensity of dental diseases using a unified approach and methodology for recording diseases of hard dental tissues.
Dental caries indices are tools that allow monitoring the prevalence and intensity of caries, determining the population's need for various types of therapeutic and preventive care, and analyzing the effectiveness of preventive programs among various population groups. Thus, in experimental analytical epidemiology it is necessary to use reliable and valid tools for assessing dental caries, providing a scientifically based assessment of community prevention methods.
When conducting epidemiological studies of caries, most researchers use the indexes of dental cpu/cpu, developed by Klein, Palmer and Knutson in 1938, as the main methods [30]. The World Health Organization (WHO) has adapted this index to conduct national dental epidemiological studies around the world [13, 24,38].
During the period 1996–1998 and 2007–2008, with the support of WHO, two national epidemiological dental surveys were conducted in Russia, where dental caries was assessed using the index KPU/KPU. There are a number of reasons why the KPU/KPU index continues to be actively used in dental epidemiological studies both in the territory of the Autonomous Okrug and in other regions of the Russian Federation [3, 5, 6, 9, 14, 17]. The undeniable advantages of this index include ease of use, proven validity and reliability of the method. However, as the tasks of caries research become more complex, a number of shortcomings of this method and new requirements for it have emerged. In particular, there are the following problems in using the KPU index [20, 21, 24–26]:
- the index is not sensitive to initial (preclinical) forms of caries,
- there is no division between uncomplicated and complicated forms of caries,
- does not take into account enamel caries,
- not reliable when assessing the proportions of components “K”, “P”, “U”,
- does not register fissure sealing on teeth/tooth surfaces,
- there are difficulties in assessing the “U” component in childhood when changing teeth and in patients over 40 years of age due to a significant increase in the number of extracted teeth due to periodontal diseases,
- The activity of the carious process is not recorded.
From the point of view of public health, the main disadvantage of the index is the registration of the carious lesion within the dentin, while the initial forms of caries and enamel caries are not described and the tooth is considered “free from caries”. The development of initial forms of caries can be stopped with the help of certain preventive measures, for example, the correct use of fluorides or the implementation of various schemes for remineralizing therapy of hard dental tissues. Consequently, a modern caries registration system should describe its various forms in order to plan, monitor and analyze the effectiveness of preventive measures among various population groups.
The purpose of this work is to critically review the main systems for assessing and recording dental caries developed in the last decade, in order to formulate the necessary requirements that an “ideal” dental caries assessment index should meet.
Significant Caries (SiC) index
According to WHO recommendations, the average intensity of caries in the population is calculated as the arithmetic mean of the sum of “K” (carious), “P” (filled) and “U” (extracted) teeth, divided by the number of people examined. However, the disadvantage of this calculation is the inability to reliably estimate the average intensity of caries in a population where the distribution of caries is “skewed”, when, for example, 20% of those examined account for 80% of all affected teeth. The Swedish researcher Bratthall [19] proposed the Significant Caries (SiC) index. The index is calculated based on individual KPU/KPU indices. The indicators are distributed in ascending order from minimum to maximum values in the study group. A series of values is divided into three equal parts, and in the third where the highest intensity of caries is noted, the average value is calculated, which is the SiC index. This tool was introduced to draw attention to individuals with high levels of dental caries.
Research confirms the value of using a combination of KPU/KPU and SiC indices to more accurately determine the level of caries incidence among different population groups, especially in identifying the most vulnerable of them [2, 23]. However, an important disadvantage of this index is that it represents an expanded value of the index KPU/KPU, since it has identical criteria for assessing the carious process. This leads to similar limitations in assessing the caries process among different population groups. However, the index is more meaningful for populations with both low rates of dental caries and a skewed distribution of dental caries within the population.
International Caries Detection and Assessment System (ICDAS) – I, II (International Caries Registration and Assessment System, versions I and II)
In 2001, through the efforts of a large group of epidemiologists and dental therapists, the International Caries Registration and Assessment System (ICDAS) was developed [27,28]. Based on various existing systems, as well as results obtained from literature reviews on clinical caries detection systems, an attempt was made to create a unified system for assessing dental caries [29]. Researchers believe that the use of this system will allow for more qualitative subsequent research in cariesology and will make it possible to adequately compare the results obtained, thereby fulfilling the basic requirements of evidence-based dentistry [30, 36]. The ICDAS tool includes the following components: “D” (detection/registration), which determines the stage of development of the carious process, topography and anatomy of the lesion; “A” (score) indicates the course of carious formation (obvious carious cavity or carious lesion without damage to the enamel; active carious cavity or suspended caries). The latter component includes recording of crown caries, but does not include root caries, and also excludes the assessment of caries activity due to considerable disagreement among research scientists.
In 2009, the ICDAS Coordination Council developed the second version of the ICDAS II system, which not only describes coronal caries, but also allows the registration of the crown of the tooth with restoration and caries, as well as with sealant (CARS) (Tables 1 and 2). Codes for registering coronal caries range from 0 to 6, determining the depth of the carious process until the dental pulp is involved in the carious lesion. The ICDAS website (www.icdas.org) provides detailed information on caries assessment criteria, including a multimedia training manual in English and German. In recent years, the ICDAS II system has been repeatedly successfully used in various in vivo and in vitro studies [26, 32]. The undoubted advantage of using this tool is a detailed assessment of the various stages of carious disease, including identification of the carious process in tooth enamel. Research results confirm the validity and reliability of the application of the existing system in clinical trials assessing the effectiveness of various preventive agents [26]. The disadvantages of this system include the difficulty of using the index when conducting mass epidemiological studies and additional time costs. The authors also point out significant difficulties with the presentation and interpretation of epidemiological data obtained using the ICDAS II system [24]. Moreover, the use of the ICDAS II tool in population-based epidemiological studies may lead to a significant exaggeration of the intensity of dental caries due to the frequent identification of early stages of the caries process, in particular with focal demineralization of the enamel (code 1) [24].
table 1 Description of clinical situations recorded with individual codes for assessing primary dental caries according to the ICDAS II system [28]
| Code | Description |
| 0 | Intact surface |
| 1 | Primary visual changes within the enamel (visualized only after using air to dry the surface for 5 seconds) or changes in the color of the enamel in pits or fissures, visible on a wet or dry tooth surface |
| 2 | Distinct visual changes in the enamel |
| 3 | Local violation of the integrity of the enamel without signs of dentin involvement in the carious lesion |
| 4 | Presence of dark shadow from dentin |
| 5 | Distinct carious cavity with exposed dentin |
| 6 | Extensive carious cavity with exposed dentin |
Table 2 Description of clinical situations recorded with individual codes according to ICDAS II for the assessment of restorations and sealants (CARS) [28]
| Code | Description |
| 0 | Intact surface |
| 1 | Sealant (sealant) partially covering fissures |
| 2 | Sealant (sealant) completely covering the fissures |
| 3 | Restoration made with composite material |
| 4 | Amalgam restoration |
| 5 | Stainless steel crown |
| 6 | Ceramic or gold crown/veneer |
| 7 | The restoration is missing or a defect has been identified |
| 8 | Temporary filling |
| 9 | The code is used if: the surface cannot be evaluated, the surface is excluded (96) |
| tooth removed due to carious process (97) | |
| tooth removed for reasons other than caries (98) | |
| the tooth did not erupt (99) |
Filled/Sound Teeth (FS-T) index (FS-T index)
In 1987, researcher Sheiham [37] proposed and developed a completely different index for assessing dental condition - FS-T-index (filled/intact tooth). The basis for calculating this index are teeth that have retained their functionality in the oral cavity (intact - Sound and filled - Filled). The index is calculated by summing the FT and ST components of 28 or 32 teeth.
When comparing the indexes KPU/KPU and FS-T, it should be noted that they determine different aspects of the dental system. The average value of KPU/KPU determines the level of caries incidence in the study group. The FS-T index measures dental health and functionality. Both indices can easily be calculated based on the same epidemiological data. According to a study by Namal et al. [34], the FS-T index gives a more positive picture than the KPU/KPU index. Filled teeth in this case are considered a positive component, since they perform their functions in the oral cavity for many years, while the “p/p” component in the structure of the index kpu/kpu is traditionally considered a negative component (since the tooth was treated due to caries - disease). Another advantage of the FS-T index is that subsequently treated teeth are considered as functioning teeth (the FS-T index value increases). Moreover, researchers have found that assessing the number of teeth that have retained their functions best reflects the socio-economic situation and environmental conditions of the population being studied, in contrast to the traditional KPU/KPU index [31]. This is exemplified by studies conducted in developed and developing countries around the world. The value of the KPU/KPU and FS-T indices in developed countries was higher than in developing countries [34].
It should be noted that the FS-T index can be used as a tool for assessing dental status at both the individual and population levels. Unfortunately, at the moment this index is extremely rarely used in epidemiological studies.
pufa/ PUFA-index (pulp-ulcer-fistula-abscess) pufa/ PUFA-index
The reason for developing this index was the inability of the traditional KPU/KPU index to reflect the presence of chronic foci of infection in the oral cavity. Complications of dental caries can cause the development of acute and chronic inflammatory diseases of the maxillofacial area. In 2009, a team of authors developed the pufa/PUFA index to more accurately determine the clinical condition of the oral cavity in children and the ability to record complicated forms of caries [33]. The clinical examination uses only a visual assessment of the tooth without the use of a periodontal/dental probe. The index makes it possible to register both temporary and permanent teeth and includes the following conditions (component p/P - complicated forms of caries, u/U - traumatic lesions of the oral mucosa, f/F - fistulous tract from the affected tooth, a/A - inflammation of the jaw bone or periosteum) (Table 3). If one of the above clinical conditions is recorded on a tooth, it is assigned a code of 1, while in the absence of symptoms, the tooth is assigned a code of 0. The pufa/PUFA index is calculated as the sum of teeth with code 1. Accordingly, the maximum index value for assessing permanent dentition is 32 points, while when determining the index value in the temporary dentition it can vary from 0 to 20 points. In many developing countries, access to dental care is limited, resulting in poor oral health care. Often, carious cavities are left without appropriate treatment or teeth are removed for urgent reasons. The advantages of this index include ease of use, as well as the ability to register temporary and permanent teeth. The obtained data can be presented separately from the KPU/KPU index. However, the results of recent studies indicate the advisability of combining the u/U code (traumatic injury to the oral mucosa) due to the very rare occurrence with the a/A code (inflammation of the jaw bone or periosteum). Thus, the reliability and validity of this method require further discussion and additional epidemiological studies [24].
table 3. Description of clinical situations recorded with individual codes for the PUFA/pufa index [33]
| Code | Name | Description |
| P/p | Pulp | Complicated forms of caries, in which the dental pulp is involved in the carious lesion and/or the coronal part of the tooth is significantly destroyed and only roots or root fragments are preserved |
| u/u | Ulcer | Traumatic lesions of the oral mucosa (fragments of the root of a destroyed tooth can injure the surrounding soft tissues - tongue, buccal mucosa) |
| F/f | Fistula | The presence of a fistulous tract from the affected tooth, where the dental pulp is involved in the carious lesion |
| A/a | Abscess | Inflammation of the bone tissue of the jaw or periosteum in the projection of the affected tooth, where the dental pulp is involved in the carious lesion |
Caries Assessment Spectrum Treatment Index (CAST) index (CAST index)
In 2011, a group of researchers from the dental schools of Radboud University (Netherlands) and the University of Brasilia (Brazil) developed a new dental caries assessment system, the Caries Assessment Spectrum Treatment Index (CAST), for epidemiological studies [24]. The use of this technique allows us to obtain more accurate data on the structure of the incidence of dental caries, as well as more detailed assessment of the effectiveness of implemented therapeutic and preventive measures in the population.
The Dental Caries Spectrum Assessment Index using the CAST method consists of ten unambiguous codes arranged in a hierarchical order. The index contains elements of previously developed systems for assessing caries disease, such as ICDAS II and the pufa-PUFA index. In particular, the pufa-PUFA index takes into account such criteria as p/P - complicated forms of caries, f/F - fistulous tract from the affected tooth, as well as the components of the index kpu/kpu - “y” and “p”.
This index is intended for use for epidemiological purposes and describes the following stages of dental disease: absence of caries formation (intact surface), prevention of occlusal caries (sealing), treatment of caries - restoration, carious lesions of enamel and dentin, tooth damage involving the pulp, abscess/fistula progress and tooth extraction (Table 4). Each tooth surface is assessed visually, without the use of compressed air to dry the patient's tooth surfaces. This is an undeniable advantage of using this system in epidemiological studies, where it is not always possible to provide the researcher with a dental unit or a portable device for supplying compressed air. Thanks to the inclusion of code 8 (tooth removed due to caries), it became possible to compare the results of assessing the spectrum of dental caries using the CAST system and the KPU/KPU index. Moreover, the inclusion of codes 6 and 7, which describe the clinical symptoms of complications of caries disease, allows comparison of the results of studies with the pufa/PUFA index. However, the CAST index is a new tool and requires confirmation of its reliability in clinical and experimental studies [24].
table 4 Description of clinical situations recorded with individual codes for the CAST index [24]
| Characteristic | Code | Description |
| Healthy | 0 | Intact surface/no visible signs of caries |
| Sealing | 1 | Pits and/or fissures are at least half covered with sealant/sealant |
| Restoration | 2 | Carious cavity restored with restoration material |
| Enamel | 3 | A distinct visual change in color/structure only within the enamel. Discoloration of enamel associated with the initial carious process, with/without localized damage to the enamel |
| Dentine | 4 | Internal discoloration of dentin associated with the carious process; discolored dentin is visualized through the enamel, which may or may not indicate visible localized enamel destruction |
| 5 | An obvious carious cavity or distinct softening of the bottom or wall of the tooth without involvement of the tooth cavity in the carious process | |
| Pulp | 6 | Deep carious formation with clear involvement of the tooth cavity (coronal pulp) or only the presence of tooth root fragments |
| Abscess | 7 | Inflammation of the bone tissue of the jaw or periosteum in the projection of the affected tooth |
| Deleted | 8 | The tooth was removed due to destruction by caries |
| Other | 9 | The code is used when it is impossible to identify/examine a tooth due to any reason |
Despite the fact that modern systems for assessing dental caries make it possible to register the disease at different stages, there are still many contradictions in the measurement and assessment of the carious process in the tooth. To date, many indices have been developed to assess caries, but none of them can be considered ideal, capable of replacing the KPU/KPU index proposed by WHO. Further development of cariesology requires the creation of a unified system for assessing the carious process with criteria that can be used both in science and in dental education and practice.
Bibliography.
- Antonova A.A., Ryabkova V.A., Talovskaya V.S. The influence of ecotoxins is a risk factor for the development of dental diseases // Pediatric dentistry and prevention. 2006. No. 3–4. pp. 11–13.
- Bazin A.K., Chebakova T.I., Zhelezny P.A., Borodina T.V., Zhezeznaya A.P., Rusakova E.Yu., Sergeeva I.L., Chebakov I.N. Epidemiological aspects of carious diseases among schoolchildren of Novosibirsk // Siberian Medical Review. 2011. T. 71, No. 5. pp. 45–49.
- Borchalinskaya K.K. Environmental risk factors for dental caries and periodontal diseases in 12-year-old children // Dental Forum. 2006. No. 1. pp. 32–35.
- Vilova T.V., Alekseeva O.V. Ecogenies and dental pathology // Human Ecology. 2006. No. 6. pp. 12–17.
- Danilov E. O., Zhapakova R. N. Study of dental morbidity in the child population of St. Petersburg according to an epidemiological survey // Childhood Dentistry and Prevention. 2008. T. 7, No. 4. P. 3–5.
- Drachev S.N., Yushmanova T.N., Ipatov O.N. Assessment of dental health of 12-year-old children living in areas with different environmental stress // Human Ecology. 2008. No. 9. pp. 33–36.
- Drachev S.N., Yushmanova T.N., Ipatov O.N. Dental aspects of the health of the adult population living in areas of environmental risk // Human Ecology. 2008. No. 2. pp. 14–16.
- Ivanova E. N. Dental caries and its prevention in conditions of biogeochemical excess of fluorine and molybdenum: abstract. dis. ...Dr. med. Sci. Moscow, 1996. 34 p.
- Kuzmina E. M., Kuzmina I. N., Petrina E. S. Dental morbidity in the population of Russia. Condition of periodontal tissues and oral mucosa / ed. prof. Yanushevich O. O. M., 2009. 224 p.
- Polozhentseva A.I., Shirinsky V.A. Influence of environmental, hygienic and socio-demographic factors on dental morbidity in the population // Human Ecology. 2012. No. 6. pp. 48–53.
- Sidorov P.I., Gudkov A.B. Human ecology in the European North of Russia // Human ecology. 2004. No. 6. pp. 15–21.
- Sovershaeva S. L., Skrebtsova N. V., Zubatkina O. V., Budyak V. P. The problem of health of residents of the Russian North // Human Ecology. 1997. No. 4. pp. 17–19.
- Kuzmina E. M., Vasina S. A., Kuzmina I. N. Modern criteria for assessing dental status during an epidemiological survey of the population. M., 2007. 32 p.
- Kuzmina E. M. Dental morbidity in the population of Russia. M., 2009. 236 p.
- Farnieva O. A., Alikova Z. R. Prevalence and intensity of caries in various ecological zones of North Ossetia - Alania // Vladikavkaz Medical and Biological Bulletin. 2010. T. 11, No. 18. pp. 119–126.
- Kharkova M.D. Efficiency of caries prevention under the influence of unfavorable environmental factors: abstract of thesis. dis. ...cand. med. sc. Minsk, 1998. 15 p.
- Yushmanova T. N., Davydova N. G. Dental health of the population aged 35–44 years living in the European North // Human Ecology. 2003. No. 1. pp. 32–35.
- Braga M. M., Oliveira L. B., Bonini G. A., Bőnecker M., Mendes F. M. Feasibility of the International caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria // Caries Research. 2009. N.43. P. 245–249.
- Bratthall D. Introducing the Significant Caries Index together with a proposal for a new oral health goal for 12-year-olds // International Dental Journal. 2000. N 50. P. 378–384.
- Broadbent J. M, Thomson WM For debate: problems with the DMF index pertinent to dental caries data analysis // Community Dental Oral Epidemiology. 2005. N 33. P. 400–409.\
- De Amorin RG, Figueiredo MJ, Leal SC Caries experience in a child population in a deprived area of Brazil, using ICDAS-II // Clinical Oral Investigation. 2012. N 2. P. 513–520.
- Diniz M. B, Rodrigues J. A, Hug I., Cordeiro RC, Lussi A. Reproducibility and accuracy of the ICDAS-II for occlusal caries detection // Community Dental Oral Epidemiology. 2009. N 72. P. 399–404.
- Ditmyer M., Dounis G., Mobley C., Schwarz E. Inequalities of caries experience in Nevada youth expressed by DMFT index vs. Significant Caries Index (SiC) over time // BMC Oral Health. 2011. N 11. P. 12–21.
- Frencken JE, Amorim RG, Faber J., Leal SC The Caries Assessment Spectrum and Treatment (CAST) index: rational and development // International Dental Journal. 2011. N 61. P. 117–123.
- Hiremath SS Indices // Textbook of preventive and community Dentistry. 2. ed. India: Elsevier; 2011. P. 198–221.
- Honkala E., Runnel R., Honkala S., Olak J., Vahlberg T., Saag M. Measuring dental caries in the mixed dentition by ICDAS // International Dental Journal. 2011. P. 150424.
- International Caries Detection and Assessment System Coordinating Committee: Criteria Manual. International Caries Detection and Assessment System (ICDAS II). Baltimore - Maryland USA, 2005. P. 43
- Ismail AI, Sohn W., Tellez M., Amaya A., Sen A., Hasson H. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries // Community Dental Oral Epidemiology. 2007. N 35. P. 170–178.
- Ismail AI Visual and visuo-tactile detection of dental caries // Journal of Dental Research. 2004. N 83. P. 56–66.
- Klein H., Palmer C. Studies on dental caries vs. familial resemblance in the caries experience of siblings // Public Health Report. 1938. N 53. P. 1353–1364.
- Maizels J., Maizels A., Sheiham A. Sociodental approach to the identification of dental treatment-need groups // Community Dental Oral Epidemiology. 1993. N 21. P. 340–346.
- Mitropoulos P., Rahiotis C., Stamatakis H., Kakaboura A. Diagnostic performance of the visual caries classification system ICDAS II versus radiography and micro-computed tomography for proximal caries detection: An in vitro study // Journal of dentistry. 2010. N 33. P. 859-867.
- Monse B., Heinrich-Weltzien R., Benzian H., Holmgren C., van Palenstein Helderman W. PUFA – An index of clinical consequences of untreated dental caries // Community Dental Oral Epidemiology. 2010. N 38. P. 77–82.
- amal N., Vehid S., Sheiham A. Ranking countries by dental status using the DMFT and FS-T indices // International Dental Journal. 2005. N 55. P. 373–376.
- Peterson PE World Oral Health Report – 2003 // Community Dental Oral Epidemiology. 2003. N 31. Supplement 1. P. 3–24.
- Richards D. Outcomes, what outcomes? (Editorial) // Evidence Based Dentistry. 2005. N 6. P. 1.
- Sheiham A., Maizels J., Maizels A. New composite indicators of dental health // Community Dental Health. 1987. N 4. P. 407–414.
- World Health Organization. Oral health surveys – basic methods. 4 ed. Geneva: World Health Organization, 1997. P. 66.
The mechanism of development of tooth root caries
Here we will explain the risk factors leading to root caries. They are divided into 2 groups:
- Factors that influence periodontal disease are:
- Insufficient prevention, incl. hygiene, both personal and professional
- Periodontal disease itself, and associated gum recession (exposure of the root)
- Elderly age
- Anatomical features of the patient’s mouth (small vestibule, short frenulum, bite pathology)
AS A RESULT – disruption of gum attachment and exposure of the root
- Once the root is exposed, the factors that cause caries come into play.
- Poor nutrition (carbohydrates)
- Fluoride deficiency (in food and toothpaste)
- Insufficient quantity or composition of saliva
AS A RESULT – the development of caries on the root surface.
One more question remains: why does caries develop faster on the root than on the crown of the tooth?
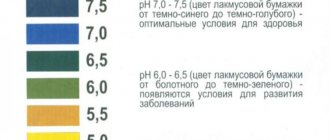
Answer: Because root cement is more sensitive to acids than highly mineralized enamel. For comparison: enamel dissolution begins at a pH less than 5.5. And cement - at 6.2 - 6.7. There is a difference?
Etiology and pathogenesis of caries
The causes of the appearance and development of caries are multifactorial, and the degree and speed of the caries process depends on a number of conditions, the combination of which leads to this disease.
Today, there are about 400 different theories explaining the etiology and pathogenesis of this disease. Among them are physico-chemical, chemical, parasitic, chemical-parasitic, biological, trophoneurotic and others. But there is indisputable evidence that caries is an infectious disease of a bacterial nature that develops as a result of the interaction of the microflora of the oral cavity with resident microorganisms of the dental plaque, forming plaque, and subsequently tartar. It has also been established that dental plaque is not able to form without the presence of a pellicle - an outer compacted layer of cytoplasm on the body surface of many protozoan organisms. The discovery of this fact has recently inclined the scientific community towards the theory of receptor adhesion in the formation of dental plaque. According to this theory, as a result of the vital activity of microorganisms living in dental plaque, organic acids are released that gradually destroy the molecular structure of the tooth. This happens as follows: consumption of carbohydrate foods and poor oral hygiene contributes to the development of pathogenic flora. Due to its constant, long-term impact on the teeth, demineralization occurs, adhesive microdamages are formed on the enamel, and cariogenic microorganisms accumulate in them, forming dental plaque. This process is carried out in several stages: the first - an hour after eating, bacteria adhesion to the pellicle occurs; second – after 24 hours, early (immature) plaque forms; third - after 72 hours, mature plaque forms; fourth – complete maturation of dental plaque and formation of dental plaque on days 3–7.
An important component of dental plaque is sugars (disaccharides, monosaccharides and microorganisms that feed on them) found in the oral cavity due to increased consumption of carbohydrate foods. The fact is that the presence of excess sugars affects the pH level (acid-base balance), causing it to deviate towards acidification or alkalization, which can become one of the factors leading to the formation of dental plaque. The speed and intensity of its development are additionally influenced by such factors as the presence of inflammatory foci in the oral cavity, the viscosity of saliva, and desquamation (flaking) of the epithelium. It is important to understand that the preservation of dental plaque on the surface of the teeth means continued exposure of organic acids to the enamel. This leads to further oxidation of the oral environment, to even greater demineralization, to a qualitative and quantitative increase in defects in the subsurface layers of enamel. But if the organic enamel matrix is preserved during the demineralization stage, caries is quite easy to stop. And then, with careful hygienic care, regular examinations in a dental clinic and remineralizing procedures, the process can be considered reversible. If demineralization leads to the dissolution of a more stable layer of enamel, caries progresses rapidly, has an increasingly destructive effect on the teeth and causes an urgent need for prompt treatment.
Thus, the nature and diet, oral hygiene, oral microflora, the percentage of fluoride in consumed water, the nature of salivation, characteristics of enamel resistance, negative effects on the body in general and the oral cavity in particular - all these factors influence the occurrence of and development of caries.
Diagnosis of root caries
Root caries is diagnosed like other diseases using basic and additional research methods:
- The main ones are questioning, inspection, probing, percussion, palpation. With their help, you can see the carious cavity on the root surface, determine its topography (on which root surface it is located), depth, edges, etc.
- Additional:
- This is an index assessment of hygiene (OHI-S, PLI), gum condition (GI, gum recession index), periodontal condition (CPI)
- Also, diagnostic tests: (saliva pH test).
- X-ray examination (bite-wing radiography, orthopantomogram)
Using X-rays, you can find hidden carious cavities under the gum, or adjacent to an adjacent tooth.
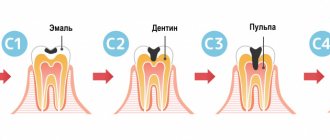
Classification of disease severity according to ICDAS
To register the status, this system also suggests using 6 codes:
- Initial focal changes in the color of the enamel surface of the tooth, which are visible only after drying.
- Clear, clearly visible changes in the enamel in the form of whitish and dark spots.
- Localized enamel lesions, which manifest themselves in limited areas of destruction.
- Destruction of enamel in a certain place along the entire thickness of its layer, down to dentin.
- The presence of a clearly visible carious cavity in the dentin.
- Severe destruction of dentin, which extends to at least half the volume of the crown.
Clinical manifestations of root caries.
The first is complaints. The patient most often complains of:
- An aesthetic defect (not beautiful) if there is caries on the vestibular surface of the front teeth.
- Discomfort while eating, pain when brushing teeth
- Symptoms of periodontal disease (bleeding gums, loose teeth, etc.)
- Short-term pain from irritants (teeth hurt from ice cream, hot tea). The pain disappears when the cause is removed.
Next, we look into the oral cavity and see the clinical picture. We will consider it taking into account the Leus classification
Along the way, root caries occurs:
- Active lesion - the edges of the cavity are undermined. The cavity is filled with softened tissues. There is a tendency towards a rapid increase in its size.
- Suspended caries - the edges of the cavity are smooth, dense, flat (not undermined). The bottom of the cavity is dense and shiny. Don't strive to get bigger.
- Secondary caries is the resumption of the process in the area of remission or after treatment (at the site of the filling).
According to the depth of the lesion:
- Without cavity formation - a white spot. Density is less than normal cement.
- With the formation of a cavity - any of those described in paragraph 1. carious defects.
Depending on what surface of the tooth it affects
Caries can affect any surface of the root, or 2 surfaces, or all surfaces in a circle (circular spread)
And lastly, according to ICD-10. There are cement caries and dentin caries.
- Cementum caries affects only the cementum of the tooth root
- Dentin caries also spreads deeper into dentin
The classification is over, and so are the clinical manifestations.
To summarize, root caries is a spot or cavity on the surface of the root of a tooth. Its edges are undermined or have smooth edges.
The cavity may be located above or below the gum.
Historical reference
It is believed that the “history” of caries begins with a change in the human diet, that is, from the time when coarse, unprocessed food began to be replaced by food subject to heat, steam and other processing, as well as from the moment when “sweets” appeared. Judging by archaeological finds, for example, by the teeth of a man who lived 13-14 thousand years ago found near the city of Lucca (Italy, Tuscany region), we can conclude that already then caries was encountered and attempts were made to treat it. In the teeth found near Lucca, cavities were found that reached the pulp, and on the walls of the teeth there were traces of drilling with some stone tools. Moreover, the teeth had fillings made of plant resin with plant fragments. This means that ancient healers tried to protect carious cavities from the penetration of food, and the plants added to the resin composition apparently served as an anesthetic.
The healers of the Mayan civilization, judging by other archaeological finds, made fillings from complex plant compositions with the addition of various minerals. In ancient Rus', caries in the initial stages was treated with honey, and in advanced stages - with propolis, which was applied to the tooth cavity, previously cleaned of decay products and affected tissues; to relieve pain, they applied a cloth soaked in a mixture of vodka and table salt. In ancient Rus', caries in the initial stages was treated with honey, and in advanced stages - with propolis, which was applied to the tooth cavity, previously cleaned of decay products and affected tissues; to relieve pain, they applied a cloth soaked in a mixture of vodka and table salt. In medieval Europe, where the development of medicine was hampered by the dogmas of the church, it was believed that caries developed due to the activity of “tooth worms”, and it was treated with poisons and hot metals introduced without anesthesia into the dental cavity affected by the disease. Moreover, these manipulations were carried out not by doctors, but by barbers. The poor people, having no means for “treatment”, received very strange, unscientific recommendations from the “doctors”: sit under the moonlight with your mouth open, tie a frog to your jaw, apply a mixture of oil and bird droppings, “rub” the affected area with the tooth of a deceased person , etc.
In the 15th century, healers began using metals, including gold, to fill teeth. In 1790, John Greenwood, the personal dentist of the first US President George Washington, came up with a primitive device for drilling teeth, where a foot drive from a spinning wheel was used to rotate the drill. More than 80 years later, in 1871, the American doctor James Morrison patented a dental drill he invented, which gave impetus to the development of therapeutic dentistry. Throughout the 20th century, therapeutic dentistry developed rapidly, adding more and more new techniques, materials and tools for the treatment of dental diseases, including caries. Today, caries treatment is the most common dental service, with high treatment effectiveness at any stage.
Treatment of tooth root caries
Treatment of root caries, as well as simple caries, begins with motivation and prevention. Read more about this in our article at the link.
Further, treatment tactics depend on the depth of the carious lesion:
Caries in the spot stage is treated with conservative retherapy. Apply:
- Fluorine preparations – varnishes, gels, solutions (Fluorine in the form of sodium fluoride, amino fluoride, tin fluoride, etc.)
- Calcium preparations (10% Calcium gluconate).
- Antiseptics (Chlorhexidine 1-2%)
Applications of these drugs contribute to the remineralization of tooth tissue, stopping and reversing the development of caries in the stain stage. Root cement (due to its porosity) is easier to remineralize than other dental tissues.
- Desynthesizers – reduce tooth sensitivity.
Caries in the stage of hard tissue defect is treated with preparation and filling.
Next, we will describe the differences between each stage of treatment.
- Disclosure. In case of root caries, the entrance to the carious cavity is wide, without overhanging edges. Therefore, no disclosure is made.
- Extension. Preventive expansion of the cavity (preparation of healthy dentin) is carried out only in case of rapidly progressing root caries.
- Necrectomy. Because the distance from the bottom of the cavity to the pulp is small, necrectomy is carried out carefully. Only softened dentin is removed.
- Formation of a carious cavity. The cavity is oval in shape. If it is located on the proximal surface, an additional platform is created on the oral one. If the cavity is located in the enamel area, create a bevel 2-5 mm wide.
- Filling. Due to the high humidity near the gum (gingival fluid), a filling material is chosen that is not afraid of moisture. This is GIC, amalgam or compomer.
And in conclusion, we summarize the main elements of the article:
- Root caries is a cavity in the root of a tooth.
- Prevalence 35.2% in the age group 55-64 years
- WHO classification – cement caries. And clinical classification of prof. Devina
- 2-stage development mechanism: root exposure + cariogenic factors
- Diagnostics - like standard caries + periodontal examination.
- Clinic: Spot caries and Cavity caries. Rapidly progressive with undermined edges and remission with a smooth surface
- Treatment: Rem. Therapy – caries spots or preparation/filling – cavity caries.
That's all. Learn, develop, read other articles. Good luck!
How to treat caries?
It is worth noting that in order to prevent the development of caries, it is recommended to visit the dentist once every six months. When the first stage of caries is detected, a high-quality filling is installed, and the carious area is removed with a drill. If caries is not treated, it progresses to more complex stages, with a large affected area, and then surgical intervention cannot be avoided. If you notice dark spots on your tooth enamel, contact your dentist immediately.
Medium caries is treated in one visit to the doctor, deep caries in 2 visits, and caries in particularly complex forms requires 3 or more visits to the clinic.
Today, caries can be treated without pain, effectively and comfortably for patients. So there is no need to delay going to the doctor. In addition to the drill, caries treatment methods include the microinvasive method, ozone therapy, air abrasive treatment and laser treatment.
WHEN SHOULD OLD FILLINGS BE CHANGED?
Replacing old fillings is a method of treating and preventing secondary caries. This makes it easier to prevent the disease from getting worse and treat it conservatively in one visit to a specialist. Therefore, old fillings that have stood for more than 5 years should be changed if:
- the tight fit of the filling to the tooth is broken, i.e. pieces of food get stuck between the material and the walls of the cavity, there is a high risk of damage to hard tissues;
- there is excess material and it “hangs” over the neighboring unit or gum, which causes a local inflammatory reaction on the gum, bleeding and the risk of destruction of the root system of the unit due to the accumulation of food and pathological microorganisms;
- abrasion of the filling has occurred, which over time leads to bite pathology and problems with the TMJ;
- The filling material did not restore the anatomy of the chewing surface, i.e. has changed the natural shape, and thus increases the risks of joint diseases;
- the aesthetics are impaired, especially the frontal group of teeth, which are visible when smiling;
It turns out that replacing fillings is important because of maintaining the health of teeth and gum tissue. If the attending physician considers it necessary to replace an outdated filling, you should agree for the sake of continued oral health.