Stages of testing the prosthesis design
After the technician has installed the artificial teeth (this was in the last article), he gives me the wax bases. Mandatory with teeth on the models and in the articulator. I, in turn, must make sure of the quality of the work. It’s just that now that the bases of the prosthesis are made of wax, any mistake will be easy to correct.
My train of thought:
1) First I evaluate working models. They should not have pores, damage or chips. Any inaccuracy on the model will make the prosthesis unbearable. So if I don't like the model, I take a functional impression again. Of course, this is difficult and unpleasant. But it will be much more unpleasant to remake a finished prosthesis.
2) The model must have markings, a midsagittal line, etc. (we talked about them in the previous article). Some anatomical features of the patient should be isolated (tori, bony protrusions, incisive papilla if it is hypertrophied). Then the base will not touch them and injure them.
3) Then I estimate the boundaries of the bases:
Firstly: they should be as thick as the edge of a functional print.
Secondly: they must fit snugly to the model throughout.
Thirdly: they must end exactly along the border of the future prosthesis
(On the upper jaw: 1-2 mm above the transitional fold, bypassing the frenulum of the upper lip and buccal cords. Distally, 1-2 mm overlaps the blind fossae (the place where the hard palate transitions to the soft palate).
On the lower jaw: 1-2 mm below the transitional fold, bypasses the frenulum of the lower lip and buccal cords and completely covers the mucous tubercle in the retromolar region. On the tongue side, the border passes through the junction of the gums and the mucous membrane of the floor of the oral cavity.)
4) I check to see if the bases are balanced.
Balancing a prosthesis is an uneven fit of the base to the prosthetic bed. The prosthesis seems to swing on the jaw.
5) I evaluate the setting of the teeth. Do they correspond to anatomical landmarks? I check whether the shape of the dentition is correct. Are there compensatory curves (Spee, Wilson). Is uniform occlusion created?
6) After a thorough check in the articulator, I remove the dentures from the models and disinfect them. After that, I put them on the patient’s jaws and test them, so to speak, in vivo.
7) First, I examine the patient’s face: is the height of the face restored, are the lips and cheeks sunken. How are the nasolabial and chin folds expressed, are the corners of the mouth drooping, and are the muscles tense?
 Then I look into the patient's mouth. I check the position of the borders of the base and make sure that they fit tightly to the mucosa. I check again to see if the prosthesis is balanced.
Then I look into the patient's mouth. I check the position of the borders of the base and make sure that they fit tightly to the mucosa. I check again to see if the prosthesis is balanced.
9) I evaluate the position of the occlusal plane. It should be parallel to the pupillary line in the anterior region and the Camper line in the area of the chewing teeth.
10) I look to see if the midline of the face coincides with the line between the central incisors, and whether each tooth has two antagonists.
11) I check if balanced occlusion is created. Those. is the same number of teeth in contact on the left and right half of the jaw for any type of occlusion (lateral, anterior).
12) I check the height of the lower part of the face. Normally, it is 2-4 mm less than the resting height. I measure the distance between two points at rest and at the position of central occlusion.
12.1) I can also use a speech test. When pronouncing the sound [v, f], the upper incisors evenly touch the lower lip. They touch it exactly along the line of transition between the lip of the face and the lip of the vestibule of the mouth (dry to wet).
If the teeth are spaced and matched correctly, the patient will not have problems pronouncing these sounds.
13) And the last thing I check is aesthetics. The upper central incisors protrude from under the lip by 1-2 mm. When smiling, the lip rises to the level of the necks of the teeth. The gums are not visible.
14) I give the patient a mirror so that he can evaluate the prosthesis himself. Only after his approval do I give the prosthesis to the technician. He exchanges wax for plastic and prepares the prosthesis for delivery.
That is if everything went well. But there may be mistakes. I'll tell you about them now.
Artificial teeth
Laminar dentures
For laminar dentures, artificial teeth are made of plastic.
There are frontal (front) and chewing (root) groups, produced in sets in headsets.
Plastic teeth are very similar in appearance to the enamel of natural teeth. During production, you can vary the color and shade. Artificial teeth are firmly connected to the base due to the homogeneity of the material (their connection occurs during polymerization of the base plastic). They are also easy to adjust both by a technician in the laboratory and by a doctor when handing over the prosthesis. Headsets are available in several styles and shades, many combinations are possible. Due to this, it is possible to harmoniously select and manufacture a prosthesis according to the individual parameters of the face.
Over time, the technology for making artificial teeth has progressed.
proposed to produce acrylic artificial teeth using the injection-compression method (continuous injection of material during polymerization to compensate for its shrinkage, followed by compaction of the material to a homogeneous state). This makes them incredibly durable.
The Ukrainian company produces artificial teeth in the form of a set in Estedent, Estedent-02. They have the following positive properties: imitation of the anatomical shape and color of the tooth; high strength indicators; fluorescent effect (both in natural and artificial lighting). Estedent-D is used for prosthetics for children during the period of temporary and mixed dentition.
“Executive” artificial teeth (“Dentsply”, USA) have five distinct shade zones, which will allow you to imitate natural teeth as accurately as possible.
Also in our country, headsets “Megastar” (Great Britain), “Ivoclar” (Liechtenstein), etc. have found use.
When selecting artificial teeth, not only the color of natural teeth (if any) is taken into account, but also the shape of the patient’s face and constitution. Thanks to a wide selection of artificial teeth in color and shape, an individual approach to each clinical case is possible.
Mistakes in the manufacture of complete removable dentures
Errors can be divided into 3 types.
- — When determining the height of the lower part of the face
- — When fixing central occlusion
- — When determining central occlusion
Errors in determining the height of the lower part of the face.
Overbite.
Why is this dangerous? With an overbite, the teeth are always in contact. The chewing muscles are tense. Because of this, there is a constant load on the prosthetic bed, which becomes injured and painful. The chewing muscles also hurt from overload. Teeth interfere with conversation and chatter. The patient has difficulty closing his lips. It is difficult to pronounce some sounds [p, b, m]. Joint damage may occur.
How to recognize? The height of the lower third of the face is too high. The difference between central occlusion and physiological rest is less than 2-4 mm. The patient has a surprised expression on his face. There are no nasolabial and chin folds. The muscles of the face and lips are tense.
What to do? If the teeth of the upper jaw are positioned correctly, you need to remove the teeth from the lower jaw, make a new bite block and determine the height of the lower part of the face (anatomically and physiologically).
If the teeth on the upper jaw are not positioned correctly (for example, they stick out from under the lip by more than 2 mm), you need to remove teeth from both jaws and make two bite ridges.
Underbite.
Why is it dangerous? The chewing efficiency of the denture decreases. Lips and cheeks are sunken. The chin protrudes forward. There may be drooling and angular cheilitis due to improper lip closure.
How to recognize? The height of the lower third of the face is reduced. The difference between central occlusion and physiological rest is more than 4 mm. The corners of the mouth look down. The nasolabial and chin folds are very well defined - an old face.
What to do? The algorithm is exactly the same as for overbite overestimation.
Errors in fixing central occlusion.
Anterior or lateral occlusions can be recorded by mistake.
Anterior occlusion was recorded.
Why is it dangerous? The denture is constantly being reset. It is impossible to wear.
How to recognize? The bite is too high. The gap between the upper and lower incisors, only the chewing teeth are in contact.
What to do? Remove teeth from the lower roller. Re-determine the central occlusion and fix it correctly.
Lateral occlusion was recorded.
It is also impossible to wear a prosthesis.
How to recognize? The bite is too high. The line between the central incisors is shifted to the left or right. On the displaced side there is no contact between the teeth. On the other side, the teeth meet cusp to cusp (lingual cusp of the lower teeth with the buccal cusp of the upper teeth).
What to do? The same as in the previous case.
Errors in determining central occlusion.
During the determination process, the base may become deformed, tear off from the prosthetic bed and move forward or backward.
Detachment of the base from the mucosa during determination of central occlusion
How to recognize? There is no contact between the teeth in any one place (where the separation occurred). You can check with a spatula. They try to insert the spatula between the antagonist teeth, but normally it does not fit through. He climbs where there was a gap.
What to do? Take a strip of wax, heat it up and place it on the artificial teeth in this place. The patient closes his mouth and the wax restores the required height. The models are re-plastered. The teeth are rearranged.
Mixing wax bases forward, backward, right or left.
How to recognize? The signs are the same as for improper fixation of the occlusion.
What to do? Teeth are removed from both jaws. Two bite ridges are made. And the central ratio is re-fixed.
Clasps
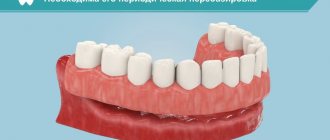
Clasp denture with clasps
In case of partial absence of teeth, one of the ways to fix the prosthesis in the oral cavity is the presence of clasps. They are usually made of metal. They tightly cover the tooth, can only serve as a retaining element, and also act as a support, that is, transmit chewing pressure to the tooth. Noticeable when talking and smiling.
Clasps made of elastic material (nylon dentures) can only perform a retaining function. Excellent aesthetics, but unreliable and can become deformed and break.
Thermoplastic materials
Recently, thermoplastic polymer materials (thermoplastics) are increasingly being used in dental practice for removable and non-removable denture structures. From the name it is clear that when heated they acquire the required shape.
These include:
- Polyamides (nylon);
- Polyoxymethylene;
- Polypropylene;
- Polyethylene;
- Monomer-free acrylates.
Nylon-based base plastics were first used in dental practice in 1954. This was a kind of attempt to improve the aesthetic parameters and convenience of the product.
Before choosing what material a removable denture , you need to know all the positive and negative aspects of each of them.
Advantages of nylon as a material for removable dentures
- Lack of so-called residual monomer - a substance that forms the basis of plastic powder and causes local allergic reactions (redness, swelling, itching of the mucous membrane of the prosthetic bed) or even systemic in some patients;
- Biocompatibility (this is important for patients with diseases of the immune, endocrine, nervous systems, and gastrointestinal tract);
- The ability to withstand enormous loads when falling, hitting or bending while maintaining the original shape (elastic deformability - elasticity) - even if you drop the prosthesis on a tiled floor, nothing will happen to it;
- Lightness and grace, subtlety;
- Strength (the ability of the prosthesis to withstand chewing pressure without destruction);
- Greater aesthetics compared to acrylic dentures (“naturalness”);
- Subjectively, for patients - greater ease of use, both during primary and repeated prosthetics (comfort, quick adaptation and invisibility to others) - “soft dentures”.
Advantages
The metal base is more durable, and the structure can serve its owner for many years without losing its performance properties. This prosthesis has other advantages:
- Reasonable price;
- Prevention of gum diseases;
- The ability to combine prosthetics with dental treatment;
- Easy maintenance of the structure;
- Possibility to leave the denture in the mouth overnight.
The prosthesis is fixed in the mouth using clasps or attachments. Clasps are hooks attached to the very base of the supporting teeth.
Device structure
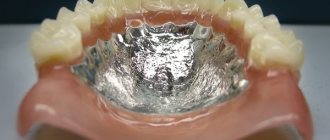
The base is made of acrylic plastic used for medical purposes. Often a metal alloy is included in the base or reinforcement is made, this allows improving the technical properties of the material:
- the strength of the apparatus increases;
- characterized by high thermal conductivity;
- has increased hypoallergenicity.
The element must have a certain structure that will guarantee long-term operation of the device and make its use more comfortable for the patient:
- for correct, uniform distribution of pressure when chewing;
- the material should minimally adsorb elements of saliva and food residues;
- a base that is convenient for easy and quick cleaning of the material with specialized means;
- strength characteristics must be high;
- the elasticity must also be sufficient, since the material is modeled under the alveolar process of the jaw arch;
- the plasticity of the apparatus should be minimal;
- an increased level of biocompatibility of the material is necessary to eliminate unwanted reactions of the body.