Removable structures
Very easy to use, they can be removed independently during meals, hygiene procedures, and if therapeutic dental treatment is necessary. Also easy to install back. There are several types:
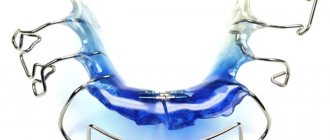
- Polymer transparent retainers-aligners, reinforced with a metal arch. They fix the position of the teeth along the length of the jaw and are invisible to others. Used constantly, excluding food intake and care procedures.
- Orthodontic plates consist of a plastic base and fixing metal elements. Basically, the designs are worn at home and put on before bed.
- Positioners keep the teeth in the correct position and restore the tone and density of the gum tissue. Made from elastic polyurethane, they are easy to use and do not cause allergic reactions. Show high effectiveness for minor occlusion disorders.
Removable orthodontic appliances are made within 3-7 days using individual impressions.
Reorganization of periodontal tissues
During orthodontic treatment, the space of the periodontal ligament expands and collagen fibers break, making it possible for the orthodontist to move the teeth.
Even if dental movement is stopped before the orthodontic appliance is removed, restoration of normal periodontal structure will not occur as long as the tooth remains in a rigid ligament with neighboring teeth, and also if it is connected to a rigid orthodontic arch. Since the teeth cannot respond to the chewing load individually, reorganization of the periodontal ligament (PDL) occurs within 3-4 months, and the slight mobility present gradually disappears when the hardware is removed.
The gingival fiber system is also destroyed during orthodontic tooth movement and must be reconstructed according to the new position of the teeth. Collagen and elastic fibers are reconstructed in the gums more slowly than in the PDS itself. The formation of a network of collagen fibers inside the gum is usually completed within 4-6 months, and the reconstruction of elastic fibers above the alveolar process is even slower, so that even a year after the removal of orthodontic equipment, forces capable of dislodging the tooth may remain.
Fixed retainers
They are represented by a thin metal arch, which is point-fixed with composite material to the inner surface of each tooth. They are installed immediately after the braces are removed, the adjustment time does not exceed a week. It must be remembered that the results of corrective treatment can only be maintained by constantly wearing retention splints! Neglecting the orthodontist's recommendations leads to deformations of the dentition and bite.
Installation Features
Retainers are installed on the day the braces are removed. Fixation is carried out after polishing the enamel and/or professional hygiene. For better adhesion, a special composition is applied to the surface of the teeth. The installation of removable devices is preceded by taking impressions and making mouth guards, positioners or orthodontic plates in the laboratory.
The final stage of treatment
Once each tooth has taken its place, therapy cannot be stopped. Indeed, over time, the curvature may develop again, and then all efforts will be useless. It is important to securely fix them in the new position. This is the main purpose of using retention devices. They must be used until the adaptation stage is completed (the period is determined by the doctor). When worn, they are imperceptible and hardly noticeable. It's not difficult to get used to them. Care does not take much time, there is no negative impact on the enamel or gums, and, as practice shows, the result is not long in coming.
General care recommendations
The retention period is the most important and integral part of the technology for correcting occlusion. The success of treatment largely depends on the patient’s conscientious adherence to the doctor’s recommendations.
- Before fixing them on the teeth, removable retainers are rinsed with a soapy solution; in the morning and before bed, it is recommended to clean them with a special brush with a low-abrasive paste. Once or twice a week, removable structures are soaked in an antibacterial solution. To protect against damage and deformation, tires should be stored in a lockable case.
- Oral care with permanently installed retainers is carried out using traditional methods. For thorough cleaning of mineralized plaque and food debris, threads, brushes, and irrigators are used.
- An indispensable condition for oral health is visiting the orthodontist at least twice a year. An emergency visit to the dentist is necessary in case of discomfort and pain, as well as in case of damage to the aligners, plates or breakage of the metal arch.
Retention devices
Retention (holding) orthodontic devices are intended to maintain the achieved therapeutic effect until complete morphological and functional restructuring, which is the prevention of relapses. The need for their use is due to the fact that the histological processes of restoration of infinitive bone tissue proceed much more slowly than the morphological and functional restructuring that was achieved during the active period of orthodontic treatment.
Retention devices must hold the tooth or jaw in a new position, minimally limit the basic functions of the oral cavity, be as aesthetic as possible, and not have a forceful effect on the dental system.
The choice of retention device design depends on the child’s discipline, parental supervision of the child, and aesthetic indications.
Retention devices can be removable or non-removable. Removable retention devices are removable plate devices for the upper or lower jaw with a plastic base with or without clasps. If necessary, vestibular arches are added to the design of the retention apparatus (Fig. 56, a). Bioplast dental aligners also give good results.
Non-removable retention devices (Fig. 56, c) are soldered rings, crowns or rings with soldered tangent beams. In some cases, industrially manufactured retainers are used (Fig. 56, b).
Medical plate devices in an inactive state can be used as retention devices. So, M.A. Napadov (1968) recommends leaving orthodontic appliances in the oral cavity as retention devices without further activation after completion of the active period of orthodontic treatment.
After treating malocclusions with an intermaxillary rubber traction, doctors often use the treatment device as a retention device, extending the period of use and weakening the rubber traction. However, a non-removable mouth guard should not be used as a retention device. Long-term use of it contributes to the occurrence of dental caries and the formation of new occlusion anomalies. It is not recommended to use an Angle arc or other arc treatment devices as a retention device, which limit the mobility of individual teeth and worsen the hygienic condition of the oral cavity (unsatisfactory cleaning of interdental spaces).
L.S. Persin (1998) recommends the use of the new OSAMU horseshoe retainer, which covers only the dental arch and part of the apical mucosa, developed by Dr. Osamu Yoshii. The retainer is made by pressing two high-quality transparent plates under pressure: soft bioplast (covering the teeth up to the alveoli) and hard-elastic Imprelon “S” (in the area of chewing surfaces).
According to G.B. Ospanova, E.V. Khazina et al. (1997) recommended the following schemes for wearing the retention apparatus: the first 3-6 months - 24 hours a day, the next 6 months every other night and then once a week. According to the authors, the orthodontist should monitor the patient for 4 years to prevent relapses.
As retention devices, the authors use elastomeric aligners, cast splinting clasps, retainers, adhesive cast structures, bracket systems with finishing arches, composite reinforced retention devices (Fiber Speint, Ribbond, standard lingual multi-link and twisted wire).
5.8. The choice of orthodontic appliance design depending on the patient’s age.
The goal of orthodontic treatment is not only to correct the position of individual teeth or the relationship of the dentition, but also to prevent “persistent correlative morphological and functional transformations based on a conditionally reflexive nature, which, naturally, is most achievable and effective with early intervention” (V. Yu Kurlyandsky).
The question of age-related indications for orthodontic treatment is the main one, since the correct answer to it is of great importance. In this regard, statements on this issue by domestic and foreign authors are of interest. The sooner defects in the teeth and dentition are eliminated, the bite is corrected, the position of the tongue and lips and the function of the oral cavity, chewing and facial muscles are normalized, the easier and faster positive treatment results are achieved in childhood.
According to Yu. B. Ginzburg, the structure of the alveolar process during growth changes under the influence of the chewing function. Before the eruption of primary teeth, the alveolar bone has a coarse fibrous structure; in the presence of temporary teeth, it becomes lamellar; during the change of teeth, osteon systems appear in it; Around the age of 20, the process of bone formation ends. Thus, orthodontic treatment is advisable at a time when the bone structure is less complex and easily amenable to influence.
According to B.N. Bynin, the most favorable period for orthodontic treatment is the period of mixed dentition. The author did not consider it possible to correct anomalies of temporary occlusion with the help of orthodontic equipment. B. N. Bynin emphasizes the inadmissibility of using any kind of mechanical equipment, much less an elastic arc, in such an early period.
Angle believed that the age of 4–6 years is favorable for the treatment of anomalies, since the facial skeleton undergoes changes even during temporary dentition and treatment at this age prepares the way for the development of a correct permanent dentition.
According to Ya.S. Khurgina, during the period of temporary occlusion, the intervention of the orthodontist should be limited to myotherapy, disorientation of the bite by grinding down the cusps, and sometimes only observation. In temporary occlusion, treatment using mechanically operating equipment is contraindicated, and the use of other equipment is ineffective due to the fact that the rudiments of permanent teeth, moved as a result of treatment along with temporary teeth, after a certain period of time (after the loss of temporary teeth) return to their original position and this causes the recurrence of deformities during the period of mixed dentition.
I.L. Zlotnik spoke out as a supporter of early elimination of anomalies. He points out that the number of relapses in the orthodontic clinic has sharply decreased, which was facilitated by the improvement of treatment methods and, to no less extent, the rejuvenation of the age composition of patients. The author recommends starting treatment for children aged 4–7 years. When treating progeny in a temporary dentition, the author advises eliminating bad habits, grinding off the cusps of temporary canines, using crowns that separate the dentition, a chin sling, and myogymnastics.
When progenizing a temporary occlusion, A.Ya. Katz recommends grinding down the cusps of the canines, and sometimes the cutting edges of the lower (temporary) incisors in order to free the lower jaw from the forced progenic state. In case of mixed dentition, the author considers it indicated to strengthen bite-dissociating crowns on the lateral teeth. When the upper teeth tilt inward or the lower teeth outward A.Ya. Katz suggests using guide crowns on the upper central incisors with extensions for the lateral incisors. The author considers it possible to use guide crowns with an inclined plane in temporary dentition. In his opinion, the only contraindication to such treatment during this period is significant mobility of the temporary incisors.
For the treatment of all types of progeny in temporary dentition E.D. Laletina used Katz guide crowns. Long-term results up to 5 years and up to 20 years showed a lasting positive effect. Based on these observations, the author came to the conclusion that correction of false progeny during the period of temporary dentition promotes the correct development of permanent dentition.
MM. Khotimskaya considers it inappropriate to prescribe functional-guiding equipment during the period of temporary occlusion - Katz guide crowns and mouthguards with an inclined plane, the use of which should be considered as a therapeutic measure, meanwhile, according to the author, self-regulation of malocclusion is possible in early childhood.
A.I. Betelman advocates starting treatment for children with malocclusions between the ages of 4 and 7 years. Our own research confirms the benefits and effectiveness of early correction of malocclusions.
V.Yu. Kurlyandsky stated that the question of the age most suitable for orthodontic treatment has not been completely resolved and will remain relevant for a long period of time. The author believed that treatment should begin soon after identifying a dental anomaly, regardless of age. To correct temporary occlusion, the author recommends the elimination of bad habits, grinding off the cusps of the teeth that prevent the correct closure of the dentition, treatment of the nasopharynx, bite separation, the application of extraoral dressings that retard the growth of the jaw bones and myogymnastics.
The point of view on the need for early treatment of children during the period of temporary occlusion finds a large number of supporters.
There is no consensus on this issue among foreign authors. Some authors (Anderson, Beker, ea) recommend orthodontic treatment of young children with temporary dentition, others (Altmann, Nord, ea) prefer to start treatment during the period of changing teeth. Korkhaus, Neumann, Oppengeim, Beichenbach and others offer a differentiated approach, namely, most authors recommend treating early (during the period of temporary dentition) true progenia, crossbite and later - at 8-10 and even 11 years - prognathia and deep bite . Higley and Skaloud attach great importance to myotherapy (special gymnastics), the founder of which should be considered Rodgers (1917). The authors emphasize the importance of proper muscle function for the development of the organs of the dental system. Prevention in infancy and early childhood is given great importance.
Treatment with a function regulator is most effective in the final period of temporary occlusion, the initial period of replacement, since during these periods there is an increase in jaw growth. Normalization of the functions of the dental system, breathing and blood circulation speeds up orthodontic treatment.
The best results of treatment with function regulators are observed at the age of 6 - 8 years. Treatment of distal occlusion with this apparatus is not indicated during the period of physiological resorption of the roots of temporary canines and their replacement. The function regulators rest on the canines, which ensures the stability of the apparatus and the distal movement of these teeth. Increased pressure on temporary canines only accelerates their loosening and loss. In such cases, it is better to use other designs of orthodontic appliances. It is advisable to begin treatment before the eruption of the second permanent molars and to use increased jaw growth in the anterior direction during this period.
The use of function regulators is indicated up to 14 - 15 years of age. However, in some cases it gives positive results even at an older age, which depends on the final timing of ossification of the skeleton.
Depending on the period of bite formation, appropriate designs of function regulators are selected. During the periods of temporary and the beginning of mixed dentition, special regulators are used (for early treatment) with wire parts resting on the occlusal surface of temporary molars. These parts prevent the adjuster from tipping over and maintain the desired bite release. When talking, swallowing, and facial expressions, the device promotes gymnastics of the muscles of the perioral area. Speech therapy exercises are of great importance - loud pronunciation of sounds, when the child is forced to close his lips and, therefore, cover the device with his lower lip.
When treating older children and adolescents with pronounced dental anomalies, preliminary removal of individual teeth is indicated. More often than other teeth, the first premolars or the first permanent molars destroyed by caries are removed.
After correcting the bite with the function regulator, a retention device is not required. The regulator can be used in the future, gradually reducing the time, which ensures the sustainability of the treatment results.
With the correct technical manufacture of the regulator, after a relatively short period of mastering it (within 1 - 11/2 months), facial expression improves. Analysis of lateral teleroentgenograms of the head showed that the regulator can be used to ensure jaw growth, teeth movement, and change in bite height.
Relapses of anomalies are observed in cases where, during the treatment, lip closure was not achieved or the bad habit was not eliminated. Normalization of the functions of the lips, cheeks and tongue is a prerequisite for the sustainability of treatment results.
Control questions:
1. Name the author of the classification of orthodontic appliances?
2. How are orthodontic appliances classified according to their operating principle?
3. How are orthodontic appliances classified according to the method and place of action?
4. How are orthodontic appliances classified by type of support?
5. How are orthodontic appliances classified by location?
6. How are orthodontic appliances classified according to the method of fixation?
7. How are orthodontic appliances classified by type of design?
8. List the main structural elements of orthodontic appliances.
9. What elements of orthodontic appliances are considered fixing?
10. What elements of orthodontic appliances are considered operational?
11. What elements of orthodontic appliances are considered auxiliary?
12. List the operating parts of functional devices.
13. How are wire mechanical elements activated?
14. How are orthodontic screws activated?
15. How long does it take to replace ligatures?
16. What are the phases of adaptation to orthodontic appliances?
17. What are the rules for choosing a support for an orthodontic apparatus?
18. What are the objectives of using retention devices?
19. What are the main designs of retention devices?
20. What are the terms of use of retention devices and the mode of their operation?
21. What are the age indications for the use of orthodontic equipment?
22. What factor determines the indications for the use of fixed orthodontic appliances?
Situational tasks:
1. Child 8 years old. The lower incisors completely overlap the upper ones. The lateral teeth occlude normally. Name the device:
A. Bruckle apparatus
B. Khurgina apparatus
C. Angle's expansive apparatus
D. Removable plate apparatus for the upper jaw with bite pads in the lateral areas.
E. Removable plate apparatus for the upper jaw with a bite platform in the frontal area.
2. Name the combined action device:
A. Kappa Bynina
B. Ainsworth apparatus
C. Bruckle's apparatus
D. Katz apparatus
E. Engle's apparatus
Advantages of the Alfa-Vid clinic
The Alfa-Vid Dental Center invites patients in need of bite correction to a free consultation. At the initial appointment, the doctor will carefully examine the oral cavity and, depending on the clinical case, will offer the best option for retention treatment. We guarantee:
- compliance with international quality and safety standards;
- individual approach;
- comprehensive problem solving.
If necessary, the patient has access to emergency assistance from doctors of related dental specialties (therapist, surgeon, etc.). The clinic is equipped with advanced European-level equipment, and dentists use high-quality materials in their work.
Why is retention needed?
- Braces have a mechanical effect on the bone and mucous tissues of the periodontal tissues, and after removing the plates, time is needed for the reorganization of these tissues.
- At the end of the course of wearing braces, the teeth are in an unstable position, pressure from the soft tissue creates a risk of relapse.
- In adolescents, changes associated with tooth growth can also cause some changes in the bite after treatment, so retainers become a necessary measure.
Basic rules of wearing and care
To maintain the results of bite correction for a long time, follow simple rules.
- Regularly undergo preventive examinations with an orthodontist to prevent displacement of teeth.
- Carefully monitor the condition of removable and non-removable structures. If they come off, become cracked, or begin to cause discomfort, consult your doctor immediately.
- When wearing permanent retainers, pay special attention to oral hygiene. Use not only a brush to brush your teeth, but also special brushes to avoid plaque accumulation in hard-to-reach places. A specialist will help you choose suitable care products.
- Remove trays and plates when eating or smoking, as food coloring and tobacco smoke can cause the plastic to become cloudy.
Retention orthodontic equipment – retainers
Retainers are needed
to keep teeth in their new place after orthodontic treatment. It is impossible not to wear a retainer, otherwise a relapse will occur. We use various types of retention devices or combinations thereof at the discretion of the treating orthodontist
- Retention plates
are removable retention devices in the form of an orthodontic plate with a plastic base and wire clasps. Made individually in the laboratory. Worn by the patient at night. Can be used in combination with a permanent retainer.
- Retention aligners
are removable biopolymer aligners that repeat the impression of the patient’s teeth immediately after completion of orthodontic treatment. Retention guards are made individually for the patient. The patient must wear the aligners every night or according to a specific pattern.
- Fixed retainers
are a thin wire that the orthodontist fixes with special glue on the inner - lingual surface of the front six teeth on the upper and lower jaw.
You will have to wear such a retainer for quite a long time - we generally recommend that our patients wear a retainer for life, but it is invisible and is not felt by the patient .
To learn more about orthodontic treatment at the GALA DENT clinic, book a consultation with our orthodontists and take advantage of all the benefits available to our patients.
Share:
Make an appointment