An inlay is a microprosthesis that fills imperfections in the crown of a tooth, which allows you to restore its shape and return the functions assigned to it. In fact, an inlay is the same filling, but performed by a technician in a laboratory.
The difference from traditional therapeutic treatment is that the material is introduced into the dental cavity not in plastic, but in solid form, which means that the inlay has visible advantages, the main of which are:
- the strength of the connection, which occurs due to the complete contact of the surfaces;
- the likelihood of restoring angles, cusps and contact points depending on age, as well as existing individual qualities;
- prevention of carious recurrence due to the constant volume of the inlay, as well as due to the precise fit;
- durability and wear resistance, which are determined by the high degree of strength of the material used;
- Due to the density of the structure, which was compiled in the laboratory, the insert does not change its color.
It is for these reasons that replacing teeth defects with inlays is a more preferable option than the usual filling.
Classification of tabs.
Tabs are classified depending on the method of expressing chewing pressure and are divided into:
- restorative. These microprostheses restore the chewing pressure that occurs on the periodontal tissues.
- loading. These structures are used for the rehabilitation of the dentition, and they are used as a support for a bridge-class denture.
- distributing. Such inserts redirect chewing pressure during teeth splinting.
Tabs are classified according to the following criteria:
Grouping of tooth cavities under inlays (according to the location of the defect).
Most often, a dental defect in the coronal lobe occurs due to caries. It is for this reason that the division of this disease according to topographic properties is of great importance.
The division was developed in 1891 by G. Black and involves dividing carious cavities into six classes depending on location. Speaking about the main advantage of this work, it should be noted the simplicity with which a doctor can use the classification.
To create the necessary conditions for fixing the tab, the doctor needs to determine which class the cavity belongs to, thereby preventing the secondary appearance of caries.
The only change that occurred with the classification can be considered the change of classes to letter definitions proposed by Boyanov in 1960. In fact, Boyanov proposed designating surfaces that have cavities.
Today the classification is as follows:
- O are cavities on the chewing planes (occlusal surfaces);
- M are cavities located on the medial plane;
- D - this is on the distal surface;
- MO are cavities that cover both the medial and occlusal surfaces;
- MOD are cavities that cover all three surfaces (occlusal, medial, and distal).
Separation by design features.
Depending on the severity of the defect in the coronal part of the tooth and how the doctor plans to place the microprosthesis, inlays replace missing tissue to varying degrees, and therefore, it is customary to distinguish four (main) types of inlay structures.
- inlay - in this design, the microprosthesis is located centrally, but at the same time does not affect the tubercles of the tooth;
- overlay - in this design, the microprosthesis covers up to three tubercles. It is worth noting that such a design, affecting four tubercles, can already refer to three-quarter crowns.
- onley - the tab touches the internal slopes, creating the effect of an overlay;
- pinley - in a similar design, a microprosthesis is strengthened in the tooth using so-called pins, that is, pins that are located in hard tissues. It is worth noting that the manufacture of such systems for chewing teeth involves covering all the tubercles. As for the front teeth, it is possible to install a pinley with full protection of the vestibular surface, as well as the incisal edge. Simply put, pinlay inlays on canines and incisors look like half-crowns with a pin.
Division depending on the material from which the inlays are made.
Depending on the material used, the tabs are divided into:
- metal models made of titanium, since this material takes root almost 100%;
- plastic inserts (nylon, acrylic, polyurethane);
- ceramic, made from materials such as zirconium, porcelain or titanium oxide;
- composite, they are also called ceramic;
- combined (metal-composite or metal-ceramic).
Depending on the chosen material, the doctor prepares the cavity for the tab and determines its features, but at the first stage, the dentist can prepare the cavity for the tab, based on the diagnosis and the drawn up treatment plan. But such an approach occurs only after a complete clinical examination.
What is IROPZ?
The root cause of damage to the integrity of the tooth remains caries.
During the pathological process, the hard tissues of the teeth are damaged, their shape is deformed, causing disruption of speech and chewing functions, and the appearance of external defects. The effectiveness of actions restoring a damaged tooth is determined by a number of factors:
- the degree of damage to the coronal area, which is under the influence of the carious process;
- timely contact with a dentist;
- correct diagnosis, professionalism and experience of specialists, as well as characteristics of the components and technological methods involved.
Before recreating the anatomical form and function of dental tissue, individual preparation is required for each individual case.
For example, the surgical effect on the hard tissues of the tooth according to Black consists of removing the enamel left without dentin and shortening the cusp damaged by more than 2/3 of the interval from the median fissure to its apex. Such an action will delay a possible fracture of the tooth crown to a later period.
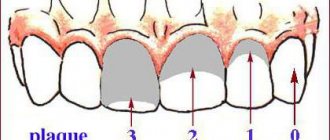
Classification of carious cavities according to Black
When crossing the contact surface with the chewing surface, it is important to try to preserve the area of Black resistance, which provides some stability to the teeth upon completion of the restoration and prevents the filling from chipping due to the load during chewing.
When calculating the coefficient of damage to the occlusion zone of chewing teeth with defects of groups 1-2 and selecting a prosthetic model, it is recommended to use the index of destruction of the occlusal surface of teeth (IROPD), developed in 1984 by the scientist Milikevich V. Yu.
Its use guarantees relatively high accuracy of experiments. Nevertheless, the method is very painstaking; its organization takes a lot of time due to the large number of its stages (taking an impression, selecting and creating a model, calculating the area and calculating the index). Recently, computer technologies have been actively used to calculate the index.
Direct methods for establishing the IROPZ index are mainly reflected in practical healthcare. These include: the visual value of IROPZ and its calculation based on anatomical indications of the occlusion surface. They are often used by specialists in the selection of options and methods of reconstruction.
Computer assessment of IRPH
IROPD in dentistry is defined as the ratio of the “cavity-filling” area to the chewing dental surface. It can be calculated by taking the total area of tooth occlusion as a unit.
With the introduction of the latest techniques and materials, the chances of recreating the coronal zone of a tooth in orthopedic dentistry have greatly expanded, and its functional significance has increased.
The selection of a tooth restoration method is influenced by:
- the existence and position of antagonists;
- degree of bite;
- oral hygiene.
Teeth are restored either by filling or prosthetics (through the use of an inlay, an artificial crown, structures with a pin), using the IROPZ index.
Based on the classification of IROPD, we can consider the main stages of damage to the hard dental membranes:
- 1st degree - from 0.2 to 0.4 - filling is used;
- 2nd degree - IROPD ranges from 0.5 to 0.6 (defect of the occlusion area is more than 50%), to prevent subsequent destruction, the inlay method should be used;
- 3 degree - index in the range of 0.6 - 0.8 (damage exceeds 60%) - filling with the involvement of artificial crowns is recommended;
- 4th degree – index value above 0.8 (destruction of the occlusion zone over 80%) – pin models and crowns are made.
In all these cases, as well as in order to avoid curvature of the dental system (with adjacent teeth with fillings recreating more than half of the chewing zone), prosthetics are recommended.
How are tabs used?
- in the form of an independent design that allows you to restore the shape, function and aesthetics of previously unsuitable crowns with IROPS indicators of 0.3–0.6, that is, in the presence of: caries, if filling turns out to be ineffective or cannot be performed;
- tissue damage of a non-carious nature, for example, with wedge-shaped defects or with increased abrasion.
IROPD - index of destruction of the occlusal surface of the tooth
It represents the ratio of the dimensions of the “cavity-filling” area to the chewing surface of the tooth.
The root cause of damage to the integrity of the tooth remains caries. During the pathological process, the hard tissues of the teeth are damaged, their shape is deformed, leading to disturbances in speech and chewing functions, and the appearance of external defects.
The effectiveness of actions restoring a damaged tooth is determined by a number of factors:
- the degree of damage to the coronal area, which is under the influence of the carious process;
- timely contact with a dentist;
- correct diagnosis, professionalism and experience of specialists, as well as characteristics of the components and technological methods involved. Before recreating the anatomical form and function of dental tissue, individual preparation is required for each individual case.
Determining the degree of destruction of the occlusal surface of the tooth is a determining factor when choosing a treatment method (filling, inlay and artificial crown) in order to prevent further destruction of crowns and tooth extraction. For quite a long time, dentists have been using the method proposed by V.Yu. to determine the area of tooth destruction. Milikevich index of destruction of the occlusal surface of the tooth.
To determine this index, the author used a standard transparent plate with a millimeter grid applied and a plaster model of the jaw. A transparent plate is applied to a plaster diagnostic model of the jaw, to the occlusal surface of the tooth with a defect, and the area of the occlusal surface and the defect is determined. Depending on this ratio, indications for replacing defects in the hard tissues of the tooth crown with various types of orthopedic structures are determined.
IROPS = Cavity/filling area / Masticatory surface area
With IROPI indicators of 0.2 – 0.4
The filling method is used. After endodontic treatment, a temporary filling (bandage) can be placed if it is not possible to place a permanent filling on the first visit or to prevent possible complications. Permanent filling is carried out in one visit.
With IROPV > 0.4
shows the manufacture of inlays from metals, ceramics or composite materials.
With IROPV > 0.6
production of artificial crowns is shown.
With IROPV > 0.8
the use of pin structures with subsequent production of crowns is shown.
Today there is a simpler and accessible way for every doctor to calculate the IRPI. We photograph the tooth from the occlusal surface using any camera (microscope, intraoral camera, camera or smartphone through a mirror) and transfer the image to the computer.
Methods for replacing dentin in restorations of lateral teeth
For more than two decades, composite restorations in the posterior region have been increasingly used as an alternative to metal ones [3]. For cavities of class I-II according to Black, in order to determine the size of the defect, doctors usually use the index of destruction of the occlusal surface of the tooth - IROPD, proposed by V. Yu. Milikevich (1984) and representing the ratio of the dimensions of the cavity-filling area to the chewing surface of the tooth. The entire area of the occlusal surface is taken as one. When the destruction index (surface area of the filling or cavity) is less than 50%, direct restoration is indicated. If IROPD is more than 50%, it is necessary to restore the tooth using an indirect method.
However, it is often difficult to motivate a patient to restore posterior teeth with a decay rate of more than 50% using indirect prosthetic restorations, such as ceramic or composite inlays [1].
An important factor in choosing between indirect and direct restoration is cost. As you know, the cost of indirect restoration is always higher than direct restoration. As a rule, in the presence of defects in the lateral group of teeth, many patients try to save money and choose cheaper treatment methods. Consequently, direct aesthetic restoration in such cases is often the ideal method to quickly solve the aesthetic problem and create a reliable, inexpensive restoration [2].
However, despite the constant improvement of composite materials, the biggest problem still remains their polymerization shrinkage, leading to a violation of the marginal fit, unsatisfactory adhesion to the cavity walls or deformation of the tubercles [3].
To solve this problem, today there are two methods: the sandwich technique and the layer restoration technique. Due to the labor-intensive, multi-stage and time-consuming procedure, the sandwich technique is not particularly popular among doctors.
Most dentists prefer to restore teeth using the layered restoration technique, that is, by combining composites with different elastic moduli (low-modulus composite as a liner, then a composite of traditional consistency). But with all this, the high polymerization shrinkage (5% or more) and low abrasion resistance of low-modulus composites do not allow their use as the main material for restoring cavities with a high C-factor [1].
The problem remains the shrinkage of composite materials, leading to a violation of the marginal fit, unsatisfactory adhesion to the walls of the cavity or deformation of the tubercles. This problem has been solved thanks to the advent of the new material “Extra Base” (VOCO, Germany) - a flowable base composite with low viscosity containing a modulator polymerization based on UDMA, which is included in the composition to reduce internal stresses (polymerization stress) caused by polymerization shrinkage. This allows it to be introduced into the cavity in layers of up to 4 mm. And it cures in just 10 seconds! In this case, there is no need to first introduce an adaptive layer of a flowable composite, since “Ex-tra Base” has a liquid consistency, so it is applied in one portion without additional condensation.
In addition, the fluid consistency ensures improved adaptation of the material to the cavity walls. "Ex-tra base" is compatible with any adhesive system and composite material based on methyl methacrylate resins. The advantage of “Extra Base” is that it has a higher content of inorganic filler than some other materials (75%) and is available in two shades (U and A2).
CLINICAL CASE
Patient T., 32 years old, came to the therapeutic dentistry clinic for the purpose of sanitation of the oral cavity. After the examination, the presence of a carious cavity with the remains of an old filling in tooth 4.7 was revealed (Fig. 1).
Rice. 1. Initial clinical situation: tooth 4.7 - there is a carious cavity with the remains of an old filling.
After receiving information about the various treatment options, the patient chose the option of a direct composite restoration using a new dentin replacement technique.
First, dental plaque was carefully removed and the carious cavity was prepared. The depth of the cavity was measured with a graduated periodontal probe, since the Ex-tra Base material can be introduced in one portion up to 4 mm thick. At the stage of necrectomy, to assess the quality of removal of non-viable dentin, the cavity was stained with a caries marker (Fig. 2).
Rice. 2. View of the cavity after adding a caries marker.
After this, all stained cavity tissue was removed using a micromotor with a ball-shaped bur (Fig. 3).
Rice. 3. View of the cavity after washing off the caries marker.
After applying the rubber dam, hard tissue was conditioned using Vococid Gel (VOCO) (Fig. 4).
Rice. 4. Stage of conditioning of hard dental tissues.
Then the cavity was washed and slightly dried using special Pele Tim foam sponges to maintain moisture in the dentin. After adhesive preparation, the flowable base composite “Extra Base” was introduced into the cavity in one portion to the enamel-dentin border (Fig. 5).
Rice. 5. Addition of the flowable base composite “Ex-tra Base”.
It was polymerized for 10 seconds. The restoration was completed by restoring the occlusal surface of the tooth using a 2 mm layer of universal composite for posterior teeth “Ex-tra fil” (VOCO, Germany) (Fig. 6).
Rice. 6. Restoration of the occlusal surface of the tooth using the “Ex-tra fil” composite.
This light-curing, radiopaque hybrid composite has been specifically developed for the restoration of posterior teeth to save time. The combination of the new multi-hybrid filler technology with the latest polymerization initiation system creates the basis of a filling material with full polymerization and very little polymerization shrinkage.
The main advantages of the “Ex-tra fil” material are: the maximum possible fullness (86% by weight) while maintaining a plastic consistency; the ability to polymerize material up to 4 mm thick with a very short exposure time of 10 seconds; increased strength characteristics. "Ex-tra fil" has one universal shade with a chameleon effect, which makes color selection easier. In addition, the material is plastic, easily modeled and adapted to the walls of the cavity, and does not stick to dental instruments.
Immediately after the restoration, finishing treatment was carried out taking into account the occlusal relationships of the teeth (Fig. 7).
Rice. 7. View of tooth 4.7 after restoration.
The importance of direct restoration with composite materials as a treatment method continues to grow steadily [3]. The use of “Ex-tra Base” and “Ex-tra Fill” composites for volumetric restoration of lateral teeth that are constantly exposed to loads makes it possible to obtain fast, durable and economical restorations. Considering the fact that only a few doctors use a rubber dam to isolate the working field during a dental appointment, the use of these materials to restore lateral teeth makes it possible to quickly create a reliable, durable restoration, which in its aesthetic characteristics does not differ from the natural structure of the tooth.
LITERATURE
- Blokhina A. Yu. Options for solving the current problem of restoring cavities in the area of the chewing group of teeth // Dentsply News. — 2011, September. - pp. 16-19.
- Goldstein R. Aesthetic dentistry. - Canada, 2003. - T. 1. - 493 p.
- Jurgen Manhart. New concept of dentin replacement in restorations of the posterior group of teeth // Densply News. — 2011, April. — P. 4-7.
NeoStom – Dentistry website
Fixed denture structures are used to replace defects in hard dental tissues, restore the anatomical shape, function of teeth and facial aesthetics. • Microprostheses: — tab — microprosthesis that restores the anatomical shape of the tooth, filling the defect in its coronal part; — veneer - microprosthesis made of ceramic or composite material, covering the vestibular, both proximal (to contact points) surfaces, and, if necessary, the cutting edge. • Artificial crowns (full and partial) - designs used in cases where restoring the shape of teeth with fillings, inlays or veneers is ineffective and impractical.• Pin structures (pin teeth, artificial crowns on a stump tab with a pin) are used when there is significant destruction of the coronal part of the tooth, when the use of an artificial crown without a pin or without a stump tab with a pin is impossible. To fix the prosthesis, the root canal of the tooth is used, in which the pin is located.
To justify the method of restoring the anatomical shape of dental crowns, clinical data such as the degree of destruction of the clinical crown, localization (topography) and size of the tooth cavity or filling are of particular importance. In the development of the carious process, its localization and depth of spread into the hard tissues of the tooth, certain patterns can be traced, determined by the histological structure of enamel and dentin, and the unequal resistance to caries of various tooth structures. The fissures of chewing teeth, contact and cervical surfaces are most often affected. Based on the patterns of distribution and typical localization of caries, G. Black in 1891 systematized the topography of carious cavities, identifying five classes: • 1st - cavities located in the fissures and natural pits of the teeth, bounded on all sides by dental tissues; • 2nd - cavities located on the mesial and distal surfaces of molars and premolars, limited by tooth tissue on three sides; • 3rd - cavities on the medial and distal surfaces of the incisors and canines with preservation of the cutting edge; • 4th - cavities on the medial and distal surfaces of the incisors and canines with partial or complete destruction of the cutting edge; • 5th - cavities on the vestibular surface in the cervical part of the tooth crowns; There is also a 6th class - cavities in the area of the tubercles of the teeth. In dental practice, the main clinical indicator when planning a method for restoring the anatomical shape of teeth is the degree of destruction of the clinical crown. Destruction of the clinical crown by 1/3, up to 2/3, and more than 2/3 is noted. These guidelines are the starting point for justifying the treatment method. Thus, when the tooth crown is destroyed up to 1/3, therapeutic methods of treatment are appropriate; from 1/2 to 2/3 - the production of inlays is shown; more than 2/3 - the use of artificial crowns. It should be noted that the criteria for clinical assessment of the degree of destruction of the coronal part are in most cases subjective, since they are based on visual assessment. The degree of destruction of the hard tissues of the crown and root of the tooth is recommended to be determined before and after the removal of all softened tissues, after which one can judge the possibility of preserving the remaining part of the hard tissues of the teeth and plan the design of the denture. For a more objective assessment of the degree of damage to hard dental tissues, the method of determining the index of destruction of the occlusal surface of the tooth (IROPD), proposed by V.Yu. Milikevich (1984). The IROPD indicator is defined as the ratio of the size of the area of a hard tissue defect or filling to the area of the chewing surface of the tooth. That is, taking the entire area of the occlusal surface as a unit, the ratio to it (as a part or percentage) of the area of the defect or the area restored with a filling (inlay) is determined: IROPD can be determined indirectly (on a diagnostic model) and directly (in the patient’s oral cavity) by methods. In the first case, to determine the surface area, a transparent plexiglass plate 1 mm thick with a millimeter grid applied to it with a division value of 1 mm2 is used. The plate is applied to the occlusal surface of the tooth with a defect on a diagnostic model of the patient’s dentition. In this case, the sides of the mesh square are aligned with the direction of the proximal surfaces of the teeth. The results are expressed in mm2 with an accuracy of 0.5 mm2. With the direct method, IROPD is determined visually, guided by anatomical formations, using a graduated dental mirror. Currently, computer technologies are used to determine the IRPI. Special programs allow you to determine the areas of objects by color and calculate indices. This technique is more objective and effective, but its practical application is limited by the cost of the hardware base, the availability of software and service capabilities. Determining the degree of destruction of the occlusal surface of a tooth is not only a diagnostic test, but also a determining factor when choosing a treatment method (filling, inlay, artificial crown or pin structure) in order to prevent further destruction of hard tissues and tooth extraction. For IROPV values: • up to 0.3, filling is indicated; • from 0.3 to 0.6 – treatment with inlays; • from 0.6 to 0.8 – treatment with crowns; • more than 0.8, the use of pin structures is indicated.
You might be interested in:
- Treatment with veneers
- Methods for making inlays
- Preparing cavities for an inlay
- Application of tabs (classification of tabs)
- Theoretical foundations of tooth preparation
Related materials:
- Examination methods for defects of hard dental tissues
- Pathology of hard dental tissues