Is it possible to diagnose a bite at home? No, but paying attention to certain deficiencies in the position of the teeth - yes, it is possible. And after that, contact an orthodontist to undergo a full diagnosis.
For self-diagnosis you will need a mirror and a little time.
It is impossible to make a diagnosis, but to suspect a problem is possible.
The condition of the bite should be assessed as follows: close your teeth tightly and open your lips slightly. Next, examine the teeth from the front and sides. There are several signs you need to pay attention to.
Jaw position and teeth closure
Normally, the lower jaw should neither protrude forward nor be pushed back relative to the upper jaw. Ideally, the upper teeth touch the lower teeth and slightly overlap them - by about a third. This means that when the teeth are tightly closed, the lower teeth will be visible.
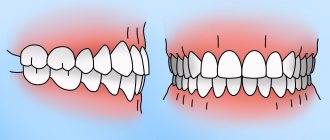
- The lower teeth are not visible at all; the upper teeth completely cover them? Perhaps it's a deep bite.
Deep bite: the lower teeth overlap the upper teeth too much, the height of the bite is reduced
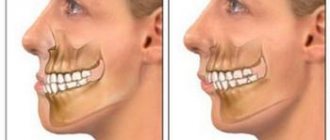
- Are the lower teeth in front of the upper teeth, especially in the anterior region (front)? Probably mesial overbite.
Mesial bite: the lower jaw is pushed forward
- The upper teeth do not overlap the lower ones, but rather touch them with their cutting edges? It appears to be a straight bite.
Straight bite: the smile may look beautiful, but the closure is incorrect and there is no overlap
- Do your upper teeth protrude too far forward, but your lower teeth cannot reach them? This happens with a distal bite.
Distal bite: the lower jaw does not reach the upper jaw
- The dentitions intersect with each other. On one side, the upper teeth protrude forward, and on the other, the lower teeth. It is imperative to consult an orthodontist, as this may be a crossbite.
Crossbite: the dentition intersects like a “scissors.”
It is necessary to examine not only the front teeth, but also the lateral teeth in a closed state. If only one lower tooth protrudes forward and covers the upper one, you can already think about a crossbite (only a doctor can make a final diagnosis).
Which prosthesis to choose if all teeth are missing?
In Russia, classical implantation is more in demand, since the immediate loading protocol is not used by all specialists due to the complexity of the procedure and subsequent prosthetics. To apply modern implantation concepts, it is necessary that the clinic meets all the requirements of the product manufacturer, and the doctor has undergone special training and internship. This requires large expenses from clinics and specialists, in addition, many patients cannot undergo the implantation procedure using the immediate loading technique due to clinical indications or due to limited budget. When choosing budget models, you cannot guarantee the result, since budget implants do not have such high reliability indicators as top manufacturers. Therefore, performing implantation in one stage when using cheap implants is a high risk for the patient. Experts do not recommend installing untested systems using the instant load protocol, since the result is unpredictable and if the operation is performed incompetently, the risk of jaw injury increases. Therefore, despite the delayed result, patients still choose the classic implantation technique for prosthetics in the absence of teeth.
When carrying out classical implantation, two stages are carried out. At the first stage, artificial roots are installed in the patient’s bone tissue, covered with a mucoperiosteal flap and sutures are applied. Without pressure or load, the implants take root in the bone ridge. When choosing budget implant models, the survival rate depends on the type of implant and the manufacturer. Modern clinics, as a rule, use high-quality products with a high degree of reliability. Engraftment occurs in 97-99% of cases when installed in two stages.
At the second stage, after complete engraftment, a gum former is installed inside the implants to create an aesthetic and natural gingival contour that will adhere to the prosthesis and cover the necks of the implants, protect against plaque formation, and prevent the development of peri-implantitis. If the fit is not precise, cavities are formed in which plaque quickly accumulates. It is difficult to remove, resulting in bad breath, inflammation of the gums, and the formation of tartar. To avoid such consequences, it is recommended to use an individual gum former, which will help create a beautiful contour and prevent the appearance of deposits between the denture and the gum.
After creating the gingival contour, the prosthesis is installed. To fix it, an abutment is used - an element connecting the implant and the prosthesis. Since the implant is completely immersed in the bone tissue, additional elements are used to fix the orthopedic structures. The abutment ensures correct load distribution over the entire surface of the implant and prosthesis. Its use prevents breakage and reduces the risk of loosening. If excessive pressure was nevertheless applied to the prosthesis, then if it breaks, only the removable part (abutment) will need to be replaced, while the implanted implant will remain undamaged.
When using a custom abutment, the bridge portion of the prosthesis can be fixed at the correct angle. Unlike standard types of abutment, when making an individual element, the angle of inclination of the prosthesis can be changed and made it most suitable for the patient. The angle of inclination determines how much load the prosthesis can withstand. For any deviations from the pressure axis, the implant and abutment will experience overload. If the lines of the abutment angle do not correspond to the natural position of the teeth and pressure on the fracture, the abutment may break when chewing hard food, even if the material is durable and made of high quality. Only if properly positioned can this element last for a long time. Standard abutment models are used if the location of the implants inside the bone allows them to be installed at a specific angle. In this case, the risk of breakdown is minimal. For this reason, implant manufacturers produce components for installing prostheses - abutments, formers, screws, plugs, etc. With a wide range of products, the doctor can select a standard product for prosthetics without risk to the patient.
The use of individual components such as an individual gum former, abutment and impression tray will allow, after installation of the prosthesis, not to experience discomfort when wearing the prosthesis, easy oral hygiene, and reduce the risk of complications.
Indications for classical dental implantation are complete or partial absence of teeth, the need to install a permanent prosthesis with permanent fixation in the oral cavity, an open palate and a natural volume of the prosthesis that corresponds to natural teeth and has an aesthetic appearance.
Contraindications to classical implantation are the presence of chronic diseases of the heart, lungs, blood, such as tuberculosis, hemophilia, oncology, type 1 diabetes mellitus, osteoporosis, disorders of bone tissue regeneration, weakened condition after a heart attack, stroke, long-term treatment. If the patient has chronic diseases that prevent surgical procedures, it is necessary to obtain additional consultation from the attending physician to eliminate the risk of complications. In the presence of atrophy, the installation of implants is contraindicated. In this case, it is recommended to undergo the procedure of osteoplasty - increasing the volume of bone tissue. After increasing the volume of the alveolar ridge, implantation can be performed. However, it is necessary to plan the procedure first of all in conjunction with the general plan for implantation and prosthetics.
Position of individual teeth
What is most striking is the uneven position of individual teeth. They can be tilted, rotated, pushed forward or pushed back relative to others.
Crowding of the upper teeth
Protrusion of teeth (excessive tilting)
Rotation of teeth (they are rotated along their axis)
If the position of the teeth is disturbed, the bite as a whole may be correct, but this is rare. Since all teeth strive to form contact, if some are deviated, others will deviate as well. Therefore, treatment is almost always required not only to straighten teeth, but also to correct the bite.
Presence of cracks
Small gaps between the teeth may not cause inconvenience and, as such, are not a malocclusion (but may accompany it).
Trema – spaces between teeth
But there can also be gaps between rows of teeth.
- Sagittal fissure: lack of contact between the lower and upper jaws in the frontal region in the direction from front to back.
Sagittal gap
That is, the front teeth do not close, and the occlusion of the lateral chewing teeth is incorrect.
- A vertical gap is a lack of contact between teeth from left to right.
That is, it is impossible to completely close the teeth; there remains a gap. It can be in the anterior section (more often) or in the lateral section (less often). If there is at least a small gap when the teeth are completely closed, the bite is considered open.
Vertical slot
Number of teeth
You need to remember whether your permanent teeth were removed and whether your wisdom teeth (eights) erupted.
- The normal number of teeth in a person is from 28 to 32.
- 28 – if not a single eight has erupted and other permanent teeth have not been removed.
- 32 – if all wisdom teeth have erupted and all teeth are preserved.
What if you have fewer than 28 teeth but have never had your permanent teeth removed? This means that either some teeth are impacted (they did not erupt and remained in the jaw in their infancy), or they do not exist at all. This condition is called partial edentia. You can find out where the missing teeth are by getting a diagnosis from an orthodontist. But most likely, if there are problems with teething, then the bite is also disturbed.
Impacted teeth in the picture
The structure of the human jaw: teeth and their formula
When citing one number for any tooth, the dentist means its anatomical and functional affiliation. If you conditionally divide the dentition into two halves and start counting from the first incisor, you will get 8 teeth in each direction (top and bottom). The first incisor is a one. The second, accordingly, is a deuce. And so on until the last molar, which is called the figure eight. If the doctor says - bottom seven on the left, then we are talking about the bottom left second molar. As you can see, everything is very simple!
This can be expressed schematically as follows (permanent teeth):
For baby teeth, everything is the same, only the teeth are designated by Roman numerals (there are no premolars in the primary dentition):
As for the two-digit designations, they were invented in order to simplify the written recording of medical history. The above is preserved, but a number appears before the number indicating which jaw and on which side the tooth is located. Conventionally, the oral cavity is divided into segments - upper right (number 1), upper left (number 2), lower left (number 3), lower right (number 4). As you noticed, the report is conducted starting from the top right and clockwise. The segment is written first, and then the tooth number. For example, the third canine from the top right would be designated tooth 13. The lower incisor on the left is 32 teeth. In children, the segments are designated by numbers 5 to 8, so as not to confuse the primary bite with the permanent one. Let's take the same third fang on the right. In a child, it will be designated as tooth 53. And so on by analogy. The main thing is to always start the report from the right side at the top, then you won’t get confused. These are not snails with 25 thousand teeth! Can you imagine their dental formulas?
Other signs
There are indirect signs of malocclusion.
- Reduced height of tooth crowns.
Typically, the front teeth are rectangular in shape. If they become square, this may be due to thinning enamel. The thickness of the enamel on the cutting edges and chewing cusps of the tooth is about 2 mm. Due to an incorrect bite, the enamel wears off and the teeth become more square in shape. This is a clear sign of an “age-related” smile, but for young people it is not the norm (unless the teeth were square from the very beginning).
Worn teeth
- Increased tooth sensitivity.
The reason is the same - the enamel becomes fragile and thin. Teeth begin to ache from hot and cold, sometimes from sour and sweet.
- Pain or clicking in the jaw joints.
They are often unnoticeable because many people eat mostly soft foods and do not spend much effort chewing. Problems with the jaw joints usually appear when trying to chew solid food. Most often, the cause of dysfunction is malocclusion. The jaws are positioned incorrectly relative to each other, so the joint is loaded unevenly.
- Discomfort when chewing or biting.
The more complex the disorder, the more noticeable it is that when chewing the load is distributed incorrectly. With an open bite, for example, some of the teeth do not close together at all, so it is difficult to chew food well.
- The symmetry of the smile is broken.
The easiest way to determine this is to look at the centers of the upper and lower jaw. They must match.
- Some teeth have a wavy edge.
The permanent teeth grow with wavy edges. And only then do they gradually grind down and become straight. This happens due to chewing. If one of the teeth is slanted or turned so that its edge is higher than all the others, it will remain wavy because it will not grind down.
Wavy edge of teeth
- The symmetry of the face is broken.
This sign needs to be assessed by looking not at the teeth, but at the face as a whole. Normally, the nasolabial folds are symmetrical. If only one of them appears, this indicates that the jaws are located asymmetrically.
- Obtuse angle between neck and chin.
If the lower jaw is too small or pushed back, a double chin may appear at a young age. This is due to the fact that due to the position of the lower jaw, the angle between the neck and chin is flattened.
Perhaps your chin looks small due to problems with your bite
If you have any doubts about the health of your teeth, consult a doctor - only an orthodontist can make a final diagnosis at an appointment, after which, if necessary, treatment can be planned.
Anatomical structure of the tooth
We figured out the order of the teeth. Further - more interesting! After all, a tooth is a unique organ, designed by nature to perform very important functions, primarily chewing. To be firmly held in the jaw bone, you need a root. The longest root is at the canine. Teeth can be single-rooted or multi-rooted. The structure of the upper teeth (molars) is somewhat more complex than that of the lower ones, since they have 3 roots. There are especially many variations in the number and type of roots in “wisdom teeth.” But the visible part of the tooth protruding above the gum is called the crown. It has different shapes in the incisors, canines and molars to perform the functions of biting, crushing or chewing food. The boundary between the crown and the root is the neck of the tooth. It is usually not visible, but it can become exposed due to certain diseases (periodontal disease, etc.). An x-ray is a kind of photo of the structure of the tooth and will give you an idea of what the state of affairs is in the oral cavity.