Chronic recurrent aphthous stomatitis (CRAS) is a chronic inflammatory disease of the oral cavity, with a high probability of relapse and recurrent rash of ulcers and aphthous stomatitis. It manifests itself in adults and children over 4 years of age and is characterized by a long course and periodic exacerbations. According to various sources, up to 20% of the planet's population is affected by the disease. Treatment is complicated by the fact that the reasons why chronic stomatitis occurs in the first place have not been fully established.
Recurrent stomatitis manifests itself in the form of small ulcers (ulcers) on the oral mucosa. There are cases where, without proper treatment, the disease persisted for several years. Aphthae are the main symptom of CRAS. As a rule, no more than 1–2 ulcers appear at a time. Painful sensations occur when talking and eating.
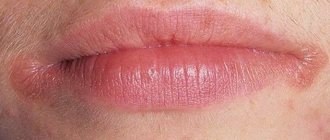
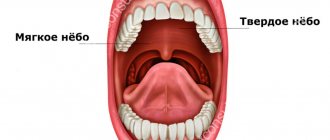
Chronic aphthous stomatitis appears periodically. At first, complications are observed mainly in spring and autumn, but then the manifestation of exacerbations becomes unsystematic. During periods of exacerbation, the mucous membrane turns pale and swells. Aphthae appear on the inner surfaces of the cheeks, mucous membranes of the lips, under the tongue on the palate or gums. Between two exacerbations it can take from several days to several years! Therefore, if you do not see canker sores for a long time, this does not mean that the disease has completely gone away.
Causes of aphthous stomatitis
- various types of allergies
- antivirus and staphylococcus
- disorders of the immune system
- neurotrophic disorders
- hereditary factors.
Scientists have not fully elucidated all the causes of aphthous stomatitis. So, if we consider chronic recurrent aphthous stomatitis as a manifestation of allergies, then its initiators can be various chemical compounds and foods to which the patient is allergic, dust, toothpaste, waste products of worms, and medications.
Necrotizing recurrent periadenitis
Necrotizing recurrent periadenitis (periadenitis mucosa necrotica recurrens), or periadenitis aphthae, recurrent aphthous cicatricial stomatitis (stomatitis aphthosa recurrens cicatricans) or Setton's aphthae. This disease is considered a more severe form of chronic recurrent aphthous stomatitis. Lesions, single or multiple, begin as small, painful submucosal nodules. Over the course of several days, they enlarge, the mucous membrane over them becomes hyperemic, then necrotic. A deep, sharply painful ulcer with raised, compacted edges is formed. Swelling and hyperemia around the ulcer are pronounced. There may be an increase in temperature and a deterioration in general condition. The ulcer heals in 3-12 weeks with the formation of a scar. The disease lasts for years, multiple scars form on the oral mucosa.
The prognosis for chronic recurrent aphthous stomatitis is favorable, but the disease is difficult to treat.
Etiology. The cause of the development of chronic recurrent aphthous stomatitis has not yet been established. Many researchers have noted the connection of this disease with other diseases - the gastrointestinal tract, liver, central and autonomic nervous system. However, chronic recurrent aphthous stomatitis can also occur in practically healthy people. The viral theory of origin, which has many supporters, still does not have sufficiently convincing evidence. Undoubtedly, changes in the reactivity of the body and its sensitization are of great importance in the pathogenesis of this disease.
Microbes and their metabolic products in foci of chronic infection can lead to allergization of the body. In chronic recurrent aphthous stomatitis, skin allergy tests with microbial allergens are usually positive for one or more allergens. The leukocytolysis reaction is also positive. A histamine skin test shows increased sensitivity to histamine. All these facts, together with the good effect of specific desensitization, indicate the great, if not leading, importance of the infectious-allergic factor in the pathogenesis of chronic recurrent aphthous stomatitis.
Histopathological examination revealed initial changes in the form of edema and perivascular infiltration in the connective tissue layer. In the styloid layer of the epithelium, vacuolization and disintegration of individual cells, spongiosis, acantholysis, microcavities, then epithelial defects and erosions occur. When areas of the minor salivary glands are damaged, infiltrates appear in the glandular tissue and along the glandular ducts, which subsequently leads to damage to the epithelium of the excretory ducts and the glandular tissue itself with the formation of foci of necrosis [Rybakov A.P., Banchenko G.V., 1978] . All layers of the mucous membrane are affected, including the submucosal layer. Around the glands, leukocyte and plasmacytic infiltration is determined.
Differential diagnosis. Chronic recurrent aphthous stomatitis should be differentiated from traumatic erosions and ulcers, chronic recurrent herpes and secondary syphilis, with aphthae in Behçet's syndrome. Ulcers in chronic recurrent cicatricial aphthous stomatitis must be distinguished from specific ulcers and cancer.
Treatment. It should begin with thorough sanitation of the oral cavity, elimination of foci of infection and exclusion of injuries, with examination of the patient by a therapist, otolaryngologist and other specialists according to indications to identify possible foci of chronic infection and their elimination.
Magnesium sulfate, sodium thiosulfate, histaglobin and vitamins are used according to the same method as for exudative erythema multiforme. In addition, a 25% solution of magnesium sulfate, 1 ml, with a 1% solution of novocaine is administered as a conduction or infiltration anesthesia (10-15 injections per course). Antihistamines give little positive results. The most effective is specific desensitizing therapy with bacterial allergens, which is carried out as with exudative erythema multiforme. Novocaine blockades of areas where aphthae appear are used with some success (for a course of 6-8 blockades every other day). In order to increase the body's defenses, prodigiosan is prescribed (0.5-1 ml of a 0.005% solution intramuscularly 2 times a week, for a course of 5 injections) or intramuscular injections of pyrogenal according to the scheme (in a hospital setting).
Patients are recommended to adhere to an antiallergic diet rich in vitamins.
Local treatment, in addition to sanitation of the oral cavity, is reduced to the use of drugs against secondary infections that promote rapid epithelization, as well as painkillers during the period of aphthalmic rash.
How to treat aphthous stomatitis
Treatment of aphthous stomatitis is the job of a qualified specialist. Self-medication is not worth it because even for a professional it is not always easy to establish the true cause of the onset and exacerbation of the disease. In general, treatment is carried out according to the following method:
- the use of medications against the ulcers themselves and to prolong remissions and prevent relapses
- the use of painkillers and necrolytic agents (to remove dead diseased tissue)
- treatment with antiseptic, anti-inflammatory and healing drugs
- referral for examination to identify concomitant and provoking diseases
- drawing up a dietary diet (necessarily excluding hot, spicy and rough foods, as well as allergens).
Aphthous stomatitis occurs not only in adults, but also in children. Moreover, the method of its treatment in children does not differ from procedures in adults. The children's diet is additionally enriched with sources of vitamins B and C, and immunostimulating drugs are prescribed.
Recurrent aphthous stomatitis of the oral cavity
Treatment is effective only with an in-depth clinical and immunological examination of patients, which allows, based on the data obtained, to select the appropriate individual complex pathogenetic therapy. Before starting treatment, the patient should be examined by a therapist, otolaryngologist and other specialists in order to identify concomitant diseases, primarily the gastrointestinal tract, foci of chronic infection, and the state of the immune system. Particular attention should be paid to identifying and treating dental and periodontal diseases.
All these measures make it possible to individualize the process of complex pathogenetic treatment, which includes the use of immunocorrective agents, metabolic correction drugs with mandatory sanitation of foci of chronic infection.
For immunocorrection, thymogen is used, which has a regulatory effect on the reactions of cellular and humoral immunity, as well as on factors of nonspecific resistance of the body. Thymogen is administered intramuscularly at a dose of 100 mcg daily for 10 days, always under the control of an immunogram before and after treatment.
To regulate the mechanisms of specific and nonspecific protection in recurrent aphthous stomatitis, levamisole (Decaris) is also used. The drug is prescribed 2 days a week (in a row or at intervals of 3-4 days, 150 mg at a time or 50 mg 3 times a day). Treatment is carried out for 1.5-2 months under the control of the clinical formula of peripheral blood and the general condition of the patient.
In order to normalize the cellular metabolism of lymphocytes, metabolic drugs are prescribed that stimulate metabolic processes at the mitochondrial level. The selection of drugs and the duration of metabolic therapy are determined by cytochemical indicators of the enzymatic status of blood lymphocytes (activity of mitochondrial sucdinate dehydrogenase, alphaglycerophosphate dehydrogenase). Prescribe 2 complexes of metabolic drugs. The first complex, used for 10 days, is aimed at activating energy processes in lymphocytes: calcium pantothenate (2 ml of a 20% solution intramuscularly or orally, 0.1 g 4 times a day); riboflavin mononucleotide (1 ml of 1% solution intramuscularly); lipamide (0.025 g 3 times a day after meals); cocarboxylase (0.05 g intramuscularly); Potassium orotate (0.5 g 3 times a day 1 hour before meals).
Over the next 10 days, a second set of metabolic drugs is prescribed that are involved in hemoglobin synthesis, regulate lipid synthesis and stabilize cell membranes: vitamin B|2 (1 ml of 0.01% solution intramuscularly); folic acid (0.005 g 3 times a day); pyridoxal phosphate (0.02 g 3 times a day after meals); methylmethionine sulfonium chloride (0.1 g 3 times a day after meals); calcium pangamate (0.05 g 3-4 times a day); phytin (0.25 g 3 times a day); Potassium orotate (0.5 g 3 times a day 1 hour before meals).
The sequence of administration of the complexes is determined by the indicators of cytochemical analysis, but, as a rule, the first complex is introduced first, optimizing the energy potential of immunocompetent cells, then the second, which requires the energy preparedness of the tissues for its utilization.
To achieve stable clinical remission of recurrent aphthous stomatitis, characterized by normalization of the cytochemical status of blood lymphocytes, 4-6 courses of metabolic correction are required at intervals of 6 months, regardless of the characteristics of the clinical course of the disease. It should be especially noted the need for metabolic therapy in the spring, when the symptoms of hypovitaminosis are pronounced, usually leading to severe exacerbations of recurrent aphthous stomatitis.
Complex therapy for recurrent aphthous stomatitis includes sedatives (valerian root, “minor” tranquilizers), glycine.
Particular attention should be paid to measures to eliminate foci of chronic infection, the sanitation of which must be carried out without fail - treatment of chronic periodontal diseases, ENT organs, gastrointestinal tract, etc. Foci of chronic sepsis cause constant bacterial sensitization, which leads to frequent exacerbations of the disease.
In order to stimulate specific and nonspecific protection factors, modern methods of physical influence on the body are effective (transcutaneous electrical neurostimulation, laser therapy on reflexogenic zones, aeroion massage on the affected oral mucosa). In severe cases of the disease, hyperbaric oxygen therapy is used.
A set of therapeutic measures, including immunocorrective, metabolic and reflexology, promotes the rapid elimination of exacerbation of the disease, significantly lengthens the periods of its remission, eliminates cellular and tissue hypoxia and normalizes immunological parameters. A positive therapeutic effect can also be obtained from each of the previously mentioned treatment methods separately, but its effectiveness is less pronounced. Therefore, it is recommended to use these methods for treating recurrent aphthous stomatitis in combination.
Diet plays an important role in successful treatment. Patients are prohibited from eating hot, spicy foods, alcoholic beverages, and smoking.
Local treatment comes down to sanitation of the oral cavity, elimination of traumatic factors and foci of chronic infection. During an exacerbation of the disease, painkillers are prescribed, since aphthae, especially ulcers, cause severe pain. For pain relief, applications of anesthetics are used (1-2% lidocaine solution, 1-2% trimecaine solution, 1-2% pyromecaine solution or 5% pyromecaine ointment), as well as a 10% suspension of anesthesin in glycerin or liquid oils (peach, apricot, sunflower).
The combined effect of medicinal and physiotherapeutic methods of pain relief is effective (microelectrophoresis on the affected area of the oral mucosa with a 2% novocaine solution followed by aeroion massage, laser irradiation).
Fibrinous and necrotic plaque from the surface of afts and ulcers is removed using proteolytic enzymes (trypsin, chymotrypsin, chymopsin, lysoamidase). Antiseptic treatment is carried out with antiseptic solutions (1% etonium solution, 0.02-0.06% chlorhexidine solution, 0.02% furatsilin solution, etc.).
To stimulate epithelization of the affected oral mucosa with recurrent aphthous stomatitis, it is advisable to prescribe an oil solution of vitamins A, E, carotolin, 5% linetol ointment, solcoseryl ointment and jelly, solcoseryl dental adhesive paste, 5% ointment and 20% Actovegin jelly, etc.
Applications and irrigation of the oral mucosa with antiseptic solutions are performed 3-4 times a day after meals. A good therapeutic effect is achieved by the use of biopolymer soluble films containing analgesic and antimicrobial drugs. To stimulate the regeneration of the oral mucosa, a sea buckthorn film containing sea buckthorn oil is successfully used.
The prognosis is favorable, especially in the case of early diagnosis and treatment of its mild form.
Acute aphthous stomatitis
The most dangerous and widespread form of the disease in children is acute aphthous stomatitis, which affects children of all ages. There are three forms: light, medium and heavy. There is an increase in temperature up to 39 degrees, the formation of many lesions in the oral cavity, ulcers and aphthae. Lesions even appear around the mouth!
If you identify the first symptoms of chronic recurrent autosous stomatitis, you should consult a doctor. Only systematic, consistent treatment can cope with the manifestations of this disease.
Healthy teeth and good health
FDC will be a pleasant find for you and your family on the path to impeccable aesthetics and good health.