Candidiasis
–
a disease of the skin, mucous membranes, internal organs, caused by the pathogenic effects of yeast-like fungi of the genus Candida, which are opportunistic microorganisms.
They are widespread in the external environment, growing mainly in the soil of meadows, gardens, on the bark of fruit trees, as well as on fruits, vegetables and fruits, especially stale ones; are easily found on household items, primarily used in caring for infants. In food production conditions, if storage rules are violated, yeast-like fungi are
constant companions of vegetable and fruit raw materials, as well as finished products.
As saprophytes, they live on the skin and mucous membranes of a healthy person. Cells of fungi of the genus Candida - blastospores - are often round, ovoid, and reproduce by budding. The formed mycelium can grow from the epithelial cell to the nucleus and cause its deformation and death. The depth of penetration of fungal elements into the affected tissues varies. Fungi of the genus Candida are aerobes. Sugars are especially readily absorbed for nutrition, which may explain the frequent candidiasis in diabetes mellitus. The optimal temperature for mushroom growth is 21-27 C, they grow well at a temperature of 37 C, a favorable pH for their reproduction is 5.8-6.5 and high humidity; drying is tolerated well; When boiled, they die within a few minutes.
The development of candidiasis is promoted by a variety of exogenous and endogenous factors. Of the exogenous influences, the most important are microtraumas and chemical damage, which not only open the gates for fungal invasion, but also disrupt the protective mantle of the skin; increased humidity and temperature, leading to maceration of the skin, especially in the folds, perianal area and external genitalia; side effects of antibiotics (both during treatment and during their production and work with them), imidazole drugs, cytostatics, corticosteroids, including when applied topically, antidiabetic drugs, oral contraceptives; chronic poisoning with nicotine, alcohol, drugs; radiation injuries. The role of endogenous factors most often is a violation of cellular immunity; diabetes; hypovitaminosis, especially due to B vitamins; intestinal dysbiosis; common serious diseases, especially cancer; chronic infections; pregnancy, gynecological diseases. The age of the patients also matters: young children and the elderly are the most vulnerable.
Oral candidiasis
Oral candidiasis – stomatitis, glossitis, pharyngitis
.
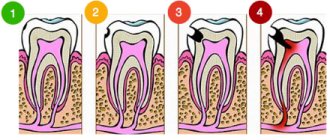
Most have no complaints. Sometimes - burning, dullness of taste, pain when swallowing. White cheesy coating on the tongue. Clinically – “thrush” – multiple white plaques in the oral cavity, on the mucous membrane of the back of the tongue, mucous membrane of the cheeks, hard and soft palate, pharynx, different in shape, 1-2 mm in size. Atrophic candidiasis
- smooth red foci of epithelial atrophy in the oral cavity - on the hard and soft palate, buccal mucosa, dorsum of the tongue; hyperplastic candidiasis - white plaques that cannot be removed; with long-term treatment with antifungal agents, the plaques gradually resolve; jam - redness and cracks in the corners of the mouth.
Lip candidiasis – cheilitis
Vaginitis, vulvovaginitis
. They begin suddenly, about a week before menstruation. Itching of the vulva, burning and pain, especially when urinating, vaginal discharge, pain during intercourse. Clinically – white curdled vaginal discharge. Swelling, hyperemia and easily removable white plaques on the mucous membrane of the vagina and cervix. Often combined with candidiasis of skin folds (perineum, inguinal folds).
Candidiasis
Candidiasis
is an infection caused by the genus Candida. The genus Candida has about 200 species that are present in food, soil, plants, and some are part of the human microflora. Several types of fungi are clinically significant, but C. albicans and C. tropicalis play a leading role in the development of candidiasis in humans.
C. albicans colonizes mucous membranes during fetal development or during the first year of life. C. albicans is present in the body of every person. Candida helps control bacteria involved in the production of vitamin K and B12, and is also involved in the breakdown of sugars. Under certain circumstances: against the background of decreased immunity, stress, a long course of antibiotic therapy and hormone therapy (including oral contraceptives), poor nutrition, the number of colonies increases and candidiasis or yeast infection develops.
Candida infection most often affects the mucous membranes of the mouth, intestines or vagina.
Candidiasis causes a wide range of symptoms: from the mildest but common forms, which are usually found in the mouth and vagina, to rare and severe forms associated with damage to the endocardium, meninges and the development of septicemia.
In accordance with ICD-10, there are:
- Candidiasis of the vulva and vagina
- Candidal stomatitis
- Pulmonary candidiasis
- Candidiasis of the skin and nails (onychia and paronychia)
- Candidiasis of other urogenital localizations
- Candidal meningitis
- Candidal endocarditis
- Candidal septicemia
- Candidiasis of other localizations
- Candidiasis, unspecified
Vulvovaginitis or vaginitis.
Also known as thrush. The disease is characterized by thick white or yellow cheesy vaginal discharge. The discharge is accompanied by itching, burning, swelling and redness of the intimate area, and an unpleasant odor. Pain and discomfort during urination or sexual intercourse are less common. Pregnant women or women with diabetes are more susceptible to the disease.
Candidal stomatitis
. The disease is characterized by the presence of ulcerative lesions and the accumulation of whitish cheesy deposits on the tongue and on the inner surface of the cheeks. The ulcers may be painful and bleed when they are scratched. Sometimes oral thrush can spread to the mouth, gums, tonsils, or the back of the throat. Candidal stomatitis can appear at any age, but is especially common in children.
Skin candidiasis
. The skin is a favorite place for the proliferation of fungi, especially in skin folds: armpits, inguinal and buttock folds, membranes between the fingers. The lesions appear as small nodules, itchy spots and reddish blisters. More often the disease develops in newborns.
Candidiasis infection of the nails (onychia) and surrounding area (paronychia)
. This form of candidiasis first manifests itself as painful swelling, which is later accompanied by the formation of pus. The infection often develops under the nail, leading to loss of the nail plate.
In addition to the main noticeable symptoms, such as thrush and a white coating on the tongue, candida has the following manifestations: craving for sweets, irritability, apathy, memory impairment, inability to concentrate and pay attention, poor sleep, mood swings, constipation, flatulence, constant feeling of fatigue .
At-risk groups
Risk groups for candidiasis include the following categories:
- children;
- overweight people;
- people diagnosed with diabetes mellitus;
- people with an underactive thyroid gland (hypothyroidism);
- people with inflammatory diseases;
- people with a weakened immune system (immunodeficiency);
- people working in wet conditions;
- pregnant women.
Protective barriers within the body
In the pathogenesis of the development of candidiasis, disturbances in the functioning of the digestive organs play an important role. There are three barriers inside the body: mechanical, physicochemical and immunobiological, which prevent the colonization of mucous membranes and skin by pathogenic microorganisms, and also cause a direct antifungal effect against candida.
The production of secretory immunoglobulin A (IgA) by the mucous membranes of the oral cavity and intestines is an immunological barrier that protects the mucous membranes from colonization by Candida fungi.
Antibacterial enzymes such as lysozyme, mucin, lactoferrin, peroxidase, found in saliva, are the first lines of defense. Long-term presence of food in the oral cavity, as well as the absence of washing it down with water or other drinks, increases the protective effect of saliva components and reduces the load on other parts of the gastrointestinal tract. The aggressive acidic environment of the stomach is the next factor of nonspecific protection. Digestion in the duodenum, the work of which equally depends on the activity of the pancreas and liver, contributes to the proper digestion of carbohydrates, fats and proteins of food and their better absorption in the small intestine. The intestine is the last authority regulating the flow of food components into the bloodstream, therefore its function, including the barrier function, will depend on the state of the enterocytes, the quality of mucin-like mucus and the presence of symbiotic flora. Treatment of candida first begins with restoring intestinal function.
The spread of candida is the result, on the one hand, of a violation of the barrier functions of the gastrointestinal tract, and on the other, the creation by the person himself of favorable conditions for the proliferation of yeast. These primarily include nutrition. One of the key factors on which 80% of the effect in the treatment of candidiasis depends is nutritional adjustments.
Nutrition
List of foods that contribute to the proliferation of candida:
- sugar and sugar-containing products;
- simple carbohydrates (baked goods, jam, preserves, carbonated drinks, ice cream);
- vegetables with a high glycemic index (potatoes);
- gluten-containing cereals;
- alcohol, caffeine.
List of products that will improve the condition of candidiasis:
- fermented foods;
- coconut oil, milk and pulp;
- ginger;
- herbal teas;
- unsweetened berries (cranberries, lingonberries);
- chia seeds, flax seeds.
Tests for candidiasis
There are several ways to detect candida directly on visible mucous membranes. To do this, a PCR study is carried out or a culture test is performed. In both cases, the subject of the study is a smear taken from the site of the lesion. Both methods determine the presence of the main culprits of the problem: fungi of the genus Candida based on the determination of DNA in the sample or the growth of a colony of fungi on a nutrient medium.
The microbiocenosis of the small intestine can be assessed using gas chromatography-mass spectrometry. The results of the analysis allow us to draw a conclusion about the state of the intestinal parietal microflora and identify which communities of microorganisms are in imbalance. The material for the study is whole venous blood.
Analysis of stool for dysbacteriosis will help to draw a conclusion about the state of the luminal microflora of the large intestine. The presence of E. coli, Klebsiella, Candida, and some types of staphylococci indicates candidiasis.
Skin candidiasis
Candidiasis of the skin, namely skin folds
: redness and itching, pustules and erosions, weeping in the armpits, inguinal, intergluteal folds, under the mammary glands.
Interdigital candidiasis
: itching, burning, erosion between the fingers and toes.
Often combined with damage to the periungual ridges and nails. Balanitis, balanoposthitis
: irritation of the glans penis, pain, burning, discharge from the cavity of the foreskin. Pustules and erosions, redness, white plaques, swelling, ulcers, cracks in the foreskin appear (usually in patients with diabetes).
Nail candidiasis
Candidiasis of nails and nail folds.
Redness and swelling of the nail folds. The swollen rollers seem to hang over the nail. When pressed, creamy pus is released from under the nail folds. Palpation is painful. Dystrophic changes in the nail plate: color change to yellow, green, black, appearance of grooves. Nail destruction. A possible complication is a purulent infection.
What is candidiasis?
Candidiasis is a group of fungal diseases of local localization and systemic nature, manifested by purulent discharge and caused by yeast-like fungi of the genus Candida.
All representatives of this genus are classified as opportunistic fungi - this means that they normally exist in the human body, but their number is strictly limited. Under certain circumstances, the fungus begins to multiply rapidly, causing the development of the disease.
This fungal infection is popularly called “thrush”, which is associated with a characteristic symptom – white discharge. Most often, the impetus for the development of the disease comes from a decrease in immunity due to stress, failure to comply with basic hygiene rules, or the introduction of a more pathogenic strain of fungi of the genus Candida, which itself begins to actively develop and stimulates the development of normal microflora fungi.
Intestinal candidiasis: symptoms, diagnosis
In 10% of the population who do not have clinical signs of fungal infection, Candida is inconsistently detected in the oral cavity, in 65% - in the intestinal contents. Under normal conditions, the main habitat of Candida in the human body is the intestines.
Clinical manifestations of intestinal candidiasis can be different:
– with manifestations of enterocolitis: complaints of spastic abdominal pain, flatulence, the presence of impurities in the stool (blood and mucus), usually there are signs of systemic candidiasis (damage to the mucous membranes of the oral cavity, genitals). Endoscopic examination reveals changes like fibrinous ulcerative colitis; – resembles a persistent course of duodenal ulcer or nonspecific ulcerative colitis, resistant to traditional therapy; – patients complain of unformed stools, flatulence, abdominal discomfort; when treated with antifungal drugs, positive clinical and laboratory dynamics are noted; – with candidiasis of the rectum, symptoms of proctitis may be observed (pain, tenesmus, pathological impurities in the stool). In some cases, this is accompanied by the phenomenon of perianal candidodermatitis.
Intestinal candidiasis is often accompanied by low-grade fever. Complications are possible in the form of the development of intestinal perforation, penetration of ulcers, bleeding, generalization with damage to parenchymal organs, and the development of fungal sepsis. Damage to parenchymal organs (liver, gall bladder, pancreas, etc.) often accompanies deep neutropenia and is observed in the terminal phase of AIDS.
Laboratory diagnostics
includes microscopic and bacteriological examination of scrapings of skin, nails, mucous membranes, scatological studies, as well as stool analysis for dysbacteriosis. In more complex situations, it is recommended to examine biopsies of the mucous membrane or skin. Recently, serological studies (antibodies) have begun to be carried out. False-positive results of serological tests are possible with mycocarriage and in healthy people sensitized by fungal antigens; false-negative tests can occur in immunodeficiency.
Risk factors for mucosal candidiasis
Defects in the antifungal resistance system briefly described above are factors contributing to the occurrence of candidiasis, or so-called. risk factors. Risk groups for the development of candidiasis of the digestive tract are presented below: • physiological immunodeficiencies (early childhood, old age, pregnancy); • genetically determined immunodeficiencies (for example, selective IgA deficiency); • iatrogenic immunodeficiencies – (for example, the consequences of treatment with glucocorticosteroids, immunosuppressants, anticytokine, radiation and polychemotherapy); • diseases of the endocrine system (for example, diabetes mellitus, autoimmune polyendocrine syndrome, hypothyroidism); • dysbiosis of mucous membranes after antibiotic therapy; • AIDS; • chronic “debilitating” diseases (for example, cirrhosis of the liver); • nutritional status disorders (for example, starvation and vitamin deficiencies).
In these groups, candidiasis is detected more often than usual. Note that sometimes the clear cause of the violation of antifungal resistance cannot be determined.
Treatment of candidiasis – intestinal and oral
There are a variety of antifungal agents: amphotericin B, itraconazole, ketoconazole, fluconazole, levorin, nystatin and natamycin (pimafucin), which can be used topically, orally and intravenously. The prescription of levorin and nystatin with a fairly high frequency is accompanied by the development of side effects (dyspeptic symptoms, allergies, toxic hepatitis).
For the treatment of intestinal candidiasis
a course of treatment with antifungal drugs is necessary for 7-10 days. Timely recognition and treatment of intestinal candidiasis is especially important as a prevention of systemic and generalized candidiasis in patients at risk, which include, first of all, patients receiving antitumor radiation and/or chemotherapy, anti-tuberculosis drugs, patients preparing for planned operations on the abdominal organs . Fucorcin solution, antifungal creams, ointments and solutions (clotrimazole, nizoral, zalain, lamisil) are used as local therapy for skin candidiasis.
For candidiasis of the mucous membranes (oral candidiasis)
– an aqueous solution of methylene blue, nystatin, suppositories with an antifungal component. For a recurrent course - oral anti-candidiasis drugs - pimafucin, nystatin, nizoral, fluconazole, itraconazole, terbinafine, as well as treatment of concomitant pathologies, immunodeficiency conditions, vitamin therapy, antioxidants, sorbents, probiotics.
dermatologist, author of the article
Antifungal resistance
The outcome of contact with yeast-like fungi of the genus Candida is determined by the state of the human antifungal resistance system. In most cases, such contact represents a transient candidal carriage, when the structures and mechanisms of antifungal resistance ensure spontaneous decontamination of the human body. At the same time, in persons with disturbances in the antifungal resistance system, contact can form both persistent carriage and candidiasis. Thus, candidiasis of the digestive tract has typical features of an opportunistic infection. The disease of candidiasis of the mucous membranes is predetermined by the presence of the so-called fungi of the genus Candida. pathogenicity factors.
In particular, fungal cells can attach to epithelial cells (adhesion), and then, through transformation into a filamentous form (pseudomycelium), penetrate the mucous membrane, even “closed” systems (invasion), and cause necrosis of the tissues of the macroorganism due to the secretion of enzymes - aspartyl proteinases and fospholipases . The listed pathogenicity factors are naturally counteracted by numerous factors of antifungal resistance. In particular, the integrity of the epithelial layer of the digestive tract and mucopolysaccharides are of great importance. The protective role is played by the antagonism of yeast-like fungi and obligate bacteria of the digestive tract, the activity of digestive enzymes and the fungistatic effect of nonspecific humoral factors, such as lysozyme, complement, secretory IgA, transferrin, lactoferrin, etc.
However, the function of phagocytic cells, primarily polymorphonuclear leukocytes, and to a lesser extent, mononuclear phagocytes and natural killer cells, is of decisive importance in the system of antifungal resistance. The specific antifungal humoral response is realized due to the synthesis by B cells of specific anti-candidal antibodies of the classes IgA, IgM, IgG and, to a certain extent, IgE. Finally, the complex cooperation of dendritic and other antigen-presenting cells, helper types 1 and 2, and regulatory cells ensures an adequate specific immune response.
Causes of candidiasis
Conventionally, the disease can be divided into childhood and adult. Infantile candidiasis can be transmitted during childbirth, by passing through infected mucous membranes of the mother, during feeding, and through everyday objects.
Due to the fact that children's immunity is poorly developed and largely depends on the mother, it is important to pay enough attention to one's own hygiene and the cleanliness of the space surrounding the child.
Adult candidiasis most often develops when the immune system is weakened, but the cause may be in factors that give impetus to the development of the disease.
Factors contributing to the development of candidiasis:
- External factors - temperature changes, humidity, skin damage, harmful environmental factors, chemical influences, leaching of one’s own microflora;
- Internal factors - metabolic disorders, non-inflammatory endocrine diseases, courses of treatment with hormonal drugs, taking hormonal contraceptives;
- Changes in the virulent properties of a fungal organism, tilting its qualities towards pathogenic ones.
Doctors note that candidiasis often occurs unnoticed by the patient, in a mild form. The body itself is able to cope with the fungus, and everything returns to normal quite quickly. However, if you notice symptoms of candidiasis, immediately contact GMS Clinic specialists to receive qualified treatment. We can provide the necessary and timely assistance to your immune system.
There are superficial and systemic candidiasis. Let's look at all types in more detail and analyze the systems of each type of candidiasis.