Halitosis
(halitosis; from Latin halitus - breath and Greek -osis - disease) or halitosis is a term used to describe a noticeably unpleasant odor when exhaling.
It is known to be the third most common reason, after tooth decay and gum disease, that prompts people to visit the dentist.
For a person with halitosis, the symptoms are invisible because the olfactory receptors become accustomed to the stench. In most cases (90%) the cause of bad breath is in the mouth.
The intensity of this phenomenon can change throughout the day due to the consumption of odorous foods such as cheese, fish, seasonings, garlic, alcohol, as well as smoking and, in general, overeating.
Since self-cleaning does not occur in the mouth during sleep, halitosis is usually more intense in the morning (“kittens wrote in their mouth”).
Bad breath can be ephemeral (going away after rinsing with a freshener or brushing your teeth) and persistent.
Sustained (chronic, persistent) halitosis is present in 25% of the population.
Causes of halitosis.
In the mouth.
There are more than 600 types of microorganisms in the average person's mouth. About a hundred of them can produce a stench even when grown in a laboratory.
Solobacterium moorei is a microorganism that is recognized by some researchers as the most active producer of stench.
This stench is produced mainly due to the decomposition of proteins into individual amino acids with their further decomposition into odorous substances.
For example, the decomposition of cysteine and methionine produces hydrogen sulfide and methyl mercaptan, respectively. Volatile sulfur compounds have been shown to be statistically related to the degree of halitosis and usually disappear with adequate treatment.
1.1. The tongue is where odor in the mouth appears in most cases.
A significant amount of natural microflora is localized in the villi and folds of the back of the tongue, especially on the back (root of the tongue).
This part of the tongue is relatively poorly cleaned and the bacterial population multiplies here on food debris, dead cells and nasal mucus.
Such a nutritional environment on the back of the tongue is ideal for anaerobic bacteria that produce a specific gas, the components of which are:
- putrid odor of indole substances,
- skatola,
- polyamines;
- “rotten egg” smell of volatile sulfur compounds (hydrogen sulfide, methyl mercaptan, allyl methyl sulfide and dimethyl sulfide).
Cleaning the tongue.
Chewing gum, sprays, rinses, etc. can only temporarily muffle the odor produced by bacteria on the root of the tongue, but cannot eliminate halitosis because they do not eliminate its cause.
To neutralize the release of the above-mentioned volatile sulfur compounds, it is necessary to remove plaque from the back of the tongue along with the aerobic and anaerobic microorganisms contained in it.
Typically, a tongue scraper or toothbrush is used for this.
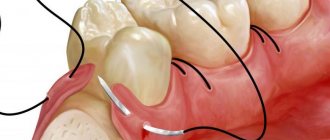
1.2. Gum diseases (periodontitis).
There is some controversy regarding the role of gum disease in the formation of bad breath. However, advanced periodontitis is always the cause of halitosis.
The waste products of anaerobic bacteria developing in periodontal pockets have a disgusting odor and, as has been clinically proven, lead to severe halitosis.
Removing calculus (tartar) and loose gums has been proven to significantly freshen the smell of your mouth. It is desirable that this event be accompanied by subgingival scaling, root planing and tissue irrigation with antimicrobial agents.
1.2.1. Particular attention should be paid to pericoronitis of the wisdom tooth.
- inflammation of the gums around the eighth tooth that has not fully erupted. After the exacerbation is relieved, it is reasonable to remove these teeth.
1.2.2.
Fetid sore throat and
Vincent's stomatitis.
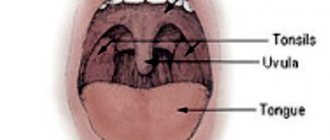
Tonsils (chronic tonsillitis).
In general, suppuration from the tonsils is considered statistically insignificant in the occurrence of halitosis (only about 5%). About 7% of the population suffers from tonsillar plugs, small pieces of calcified material in the folds of the tonsils.
They smell extremely unpleasant and when released can cause halitosis.
Nasal passages.
The nose is the second major cause of halitosis due to sinusitis and foreign bodies. In this case, the smell rather comes from the nose and is different from bad breath.
Esophagus.
The cardiac valve between the stomach and esophagus may not close well when the stomach herniates into the esophagus, allowing acid and stomach gases to leak into the mouth. With diverticulosis (false pouch) of the esophagus, deposited food debris can cause halitosis.
Stomach
Rarely is the cause of halitosis; belching should not be confused with the latter. With reflux (backward release of stomach contents), an odor may appear.
Liver.
Hepatic respiration (fetor hepaticus) is a condition associated with portal hypertension and liver failure. In this case, odorous digestive products (mercaptan, ammonia, ketones), instead of being destroyed in the liver, enter the lungs and, accordingly, into the exhaled air.
The breath has a sweetish, fecal tint. In this case, the fight against symptoms is no longer relevant.
Lungs and bronchi in acute and chronic inflammation and tumors (carcinoma).
Other diseases:
- renal failure,
- diabetes,
- metabolic diseases.
Hepatic encephalopathy - symptoms and treatment
The diagnosis of “hepatic encephalopathy” is established by characteristic clinical manifestations, results of laboratory and instrumental studies and psychometric testing data. Further treatment tactics and prognosis of the disease will depend on the degree (stage) of the disease.
Diagnosis of stages I-IV of manifest (clinically pronounced) hepatic encephalopathy is not difficult, since each stage is characterized by certain symptoms [10]. It is much more difficult to recognize the disease at the initial stage: there are no clinical symptoms during a latent course, laboratory parameters are not changed. Therefore, psychometric tests are most often used to detect minimal hepatic encephalopathy.
Recognizing the hidden course of the disease is very important for two reasons:
- firstly, minimal hepatic encephalopathy is very common (50 to 70% of cases in liver cirrhosis);
- secondly, it can lead to a traumatic situation, especially while driving a car, since at this stage of the disease the patient does not respond adequately to extreme circumstances [10][16][17][18].
Hepatic encephalopathy can be suspected in patients with the following symptoms:
- inattention, memory impairment;
- inhibited thinking;
- decreased reaction speed;
- decreased performance;
- disturbance of visual perception;
- irritability.
Laboratory diagnosis involves determining the level of ammonia in arterial blood: it is elevated in more than 90% of patients with overt hepatic encephalopathy. However, during a latent course of the disease, the ammonia concentration may be normal, so this indicator is not an exclusion criterion when making a diagnosis [18].
| Degree of hepatic encephalopathy | Arterial ammonia levels |
| 0 | Norm |
| I | Up to 1.33 from ULN* |
| II | 1.33-1.67 ULN |
| III | 1.67-2 VGN |
| IV | More than 2 ULN |
| *ULN is the upper limit of normal, equal to 60 µmol/l | |
Psychometric testing is primarily used to diagnose clinically silent hepatic encephalopathy. The sensitivity of the tests is quite high - 70-80%.
Over the past 30 years, dozens of simple, accessible psychometric tests have been developed that can be used in various combinations. They are divided into two groups:
- tests for the speed of cognitive reaction (for example, the number connection test - the most common and well-known in clinical practice);
- fine motor accuracy tests (eg line copying test).
When conducting a number connection test, the patient needs to connect the numbers from 1 to 25 with a line. They are printed randomly on a sheet of paper.
To evaluate the test, the task execution time (in seconds), including time spent correcting errors, is used [18]. The interpretation of the results is given in the table.
| Time | Points | Disease stage |
| Less than 40 s | 0 | No |
| 41-60 s | 1 | 0-I |
| 61-90 s | 2 | I-II |
| 91-120 s | 3 | II |
| More than 120 s | 4 | II-III |
The following psychometric tests are also used in the diagnosis of hepatic encephalopathy:
- handwriting recognition test;
- numbers and symbols test;
- line copy test;
- visual memory test;
- alphabetical elimination test;
- linear maze test;
- dots and circles test;
- test for memorizing a pair of words;
- star construction test;
- sequential subtraction test;
- text retelling test, etc. [16][17][18].
Instrumental diagnostics are carried out using the critical flicker frequency (CFF) method. In 2002, it was first used to diagnose minimal hepatic encephalopathy. The study is carried out using the HepatonormTM hepatoanalyzer. In this device, the patient sees what seems to him to be a constant red glow, but is actually a high-frequency flickering [13][15].
During the FFM test, the frequency of the red light, which is initially 60 Hz and is generated as a high-frequency pulse, causes the patient to feel a constant light, and then changes to flickering over time. It is at this moment that the patient needs to press a button on the device. The hepatoanalyzer records the frequency at which the red beam “began to flicker.”
The study is carried out 8-9 times. The average value of the CFM is used for evaluation. Based on the test result, the stage of hepatic encephalopathy is established: values below 39 Hz correspond to minimal hepatic encephalopathy, 35.9-32 Hz - stage I, 31.9-28 Hz - stage II, below 27.9 Hz - stage III [15].
Hepatic encephalopathy can also be diagnosed using EEG - electroencephalography. However, the validity of the results of this study may be affected by medications or decreased sodium levels in the blood [21].
If intracerebral hemorrhage is suspected or differential diagnosis is necessary, CT and MRI of the brain may be required [21].
Differential diagnosis
When diagnosing hepatic encephalopathy, it is important to exclude other causes that could cause the same clinical symptoms. Such reasons include neurological, somatic diseases and various intoxications.
Differential diagnosis is complicated by the lack of distinctive symptoms that would be found only in hepatic encephalopathy. The American Association for the Study of Liver Diseases recommends that disorders that also alter the level of consciousness be considered when making a diagnosis. These include:
- metabolic encephalopathy - associated with metabolic or electrolyte disorders, characterized by low levels of sodium and potassium in the blood or hypoglycemia;
- alcoholic encephalopathy - accompanied by intoxication, withdrawal syndrome (abstinence), developing Wernicke encephalopathy is associated with vitamin B1 deficiency;
- drug encephalopathy - caused by taking benzodiazepines, antipsychotics and opioids;
- neuroinfections - occur under the influence of bacteria, viruses, fungi or protozoa;
- intracranial hemorrhage , subdural hematoma , stroke , tumor or brain abscess - develop against the background of congenital or acquired diseases associated with circulatory disorders [10][13][18].
Diagnosis of halitosis.
Self-diagnosis.
Smelling your own breath is difficult due to the adaptation of the olfactory receptors, although many halitosis sufferers can smell it in others.
Sometimes people experience an unpleasant taste in their mouth, but this is not always accompanied by halitosis. Usually people reliably learn about the presence of halitosis from their loved ones or from their doctor.
Special diagnostics.
It is required if the possible causes of halitosis, especially in the mouth, have been eliminated.
2.1. Halitometer
This is a device that determines the amount of hydrogen sulfide in exhaled air. Other odorous agents, such as mercaptan, are not detected by this device.
2.2. Digital gas chromatograph
measures the molecular level of major halitosogenic substances.
Treatment and prevention.
1.
It is known that very few people observe sufficient personal hygiene measures necessary for fresh breath.
This is, firstly, adequate teeth cleaning using electric, sonic and ultrasonic toothbrushes and irrigators with quality control using special plaque indicators.
Secondly, it is advisable to clean the tongue with a scraper and brush. Medicinal rinses are also appropriate.
2.
Diet. When eating raw, hard vegetables and fruits, the oral cavity self-cleanses.
3.
High-quality regular, if necessary repeated, professional teeth cleaning with removal of plaque and stones using ultrasound and sandblasting (air-flo).
Sometimes deep scaling, root planing and gum margin management are required. In advanced cases, reconstructive gum surgery is used.
4.
Dental treatment and adequate dental prosthetics.
Drug therapy.
1.
Antimicrobial drugs.
2.
Probiotics. For example Streptococcus salivarius K12.
6. Traditional medicine.
Camomile tea.
Pour a teaspoon of chamomile flowers into a glass of boiling water, leave for 2 hours, strain. Rinse your mouth with freshly prepared chamomile infusion 3 times a day.
Halitosis and exposed roots
Two recent studies show that volatile chemicals and the gas that causes halitosis have damaging effects on surrounding tissue.
The first study demonstrates the role of hydrogen sulfide (SH2), which causes periodontal cell death through apoptosis (fragmentation or programmed destruction).
Another study shows that the same hydrogen sulfide (SH2) accelerates the proliferation (reproduction) of bone-destructive cells (osteocasts).
These are cells that take part in the physiological (normal) remodeling of bone: the phenomenon of bone resorption, which allows, among other things, orthodontic movements, during which the activity of bone-building cells (osteoblasts) is balanced with the activity of osteoclasts.
Under the influence of hydrogen sulfide, cellular metabolism accelerates, triggering the mechanism of bone destruction under the influence of osteoclasts.
The balance is thus disturbed and bone resorption develops. This results in periodontal disease (periodontitis) and exposed roots.
The vicious circle is complete because periodontitis and exposed roots are a common cause of halitosis (bad breath).
Halitosis and pulpitis
Hydrogen sulfide, released during halitosis (bad breath), is also toxic to pulp cells. One study demonstrates that hydrogen sulfide profoundly disrupts the metabolism of the mitochondrial membranes of dental cells, causing cell death through apoptosis (breakdown into fragments).
Situated in the pulp chamber in the center of the tooth, the pulp is not isolated from the surrounding oral environment because exchange constantly occurs through dentin, a porous tissue, and enamel, which acts as a selective membrane.
Hydrogen sulfide penetrates and diffuses through the hard tissues of the tooth to negatively affect its vitality.
This phenomenon may explain the appearance of pulpitis (inflammation of the pulp) in intact (undamaged) teeth. It should be noted that tobacco smoke can have a toxic effect on the dental pulp through a similar mechanism.
In the case of pulpitis, divitalization or removal of the nerve is the only possible solution.
What else can cause bad breath?
Bad breath is not always associated with problems in the oral cavity. It may be related to a person's lifestyle. For example, heavy smokers and “fans” of alcohol can be easily recognized by the specific odor from their breath. Bad breath can also be a syndrome of diseases of various organs and systems of the body.
What diseases cause bad breath?
Bad breath can occur when:
- Diseases of the ENT organs;
- Liver cirrhosis;
- Bronchitis, pneumonia, other diseases of the bronchopulmonary system;
- Severe kidney pathologies;
- Diseases of the gastrointestinal tract - gastroesophageal reflux, ulcers, etc.;
- Lactose intolerance, gluten intolerance and many other diseases.
Which doctors should you contact if you have bad breath?
Since halitosis is most often associated with dental reasons, you should first contact an experienced dentist. For example, at the first consultation, our clinic’s specialists will conduct a diagnosis and determine whether the problem is related to diseases of the oral cavity, and will give recommendations on how to solve it.
If it turns out that everything is in order regarding dentistry, you need to contact a therapist. After an examination and study of the medical history, he will give a referral to the appropriate doctor - otolaryngologist, gastroenterologist, endocrinologist, psychologist or other specialized specialist.