What is mandibular hyperplasia?
Hyperplasia is characterized by a constant or rapidly growing condyle when growth should be slowed or stopped. This condition causes development of the head, neck and jaw, causing significant functional and aesthetic deformities of the face. Disorders of the dental craniofacial structure affect the normal growth of the jaw, which leads to gross changes in the normal morphology and structure of the hard and soft overlying tissues. The result is asymmetry and significant functional deformities, which pose a serious problem for both orthodontists and maxillofacial surgeons.
Preventing abnormal jaw development
Long-term treatment can be avoided if changes are identified in time and preconditions for abnormal development are eliminated. To do this you should:
- wean the child from bad habits;
- promptly treat acute respiratory infections and ENT pathologies (rhinitis, adenoids, tonsillitis), avoiding frequent and prolonged mouth breathing;
- introduce solid foods in a timely manner;
- monitor posture and correct seating at the table (without asymmetry of shoulders, shoulder blades and other deviations);
- eliminate the usual incorrect position of the body and head during sleep (high headboard or tilting the head back).
A forward thrust of the lower jaw can cause unpleasant consequences, but fortunately, it can be corrected. The younger the patient, the easier it is to return the protruded jaw to its place, so it is better not to delay treatment. Adults will have to prepare themselves for long-term therapy, which requires accuracy and discipline, or for a complex surgical operation.
Causes of hyperplasia
(MG) is caused by overdeveloped, aggressive growth of the condyle. This condition causes abnormal jaw growth, which means one side of the jaw stops growing earlier. Juvenile idiopathic arthritis (JIA) and condylar fractures can cause growth and mandibular problems. Inflammatory and/or mechanical damage to the condylar cartilage often causes jaw hyperplasia.
Symptoms of inferior hyperplasia
Symptoms include slowly progressive unilateral growth of the condyle of the head and neck. This results in malocclusion, facial asymmetry, and a shift to the middle of the chin on the unaffected side. Characteristics of condylar hyperplasia may also include: a posterior open bite or tilted occlusal plane, depending on the time at which the hyperplasia develops, and asymmetry of the lower half of the face. Characteristic symptoms of lower hemisphere hyperplasia are asymmetrical facial bones (enlarged lower facial bones on one side).
Deep bite - symptoms and treatment
The goal of deep bite treatment is to provide a well-functioning and anatomically optimal occlusion (the occlusion of the upper and lower teeth) that is in harmony with the skeletal framework, is esthetically acceptable to the patient, and maintains functional stability with age [3].
There are surgical and non-surgical correction of deep bites. Non-surgical tactics include orthodontic and orthopedic methods. Orthodontic treatment involves the use of three main strategies: extrusion (progression) of the lateral teeth, vestibular inclination of the anterior teeth in combination with intrusion (vertical displacement) of the upper and/or lower incisors [2]. Orthopedic methods include the use of onlays, veneers or crowns.
Before any treatment of the bite, it is necessary to sanitize the oral cavity, i.e., eliminate all foci of chronic infection (carious cavities, periodontitis, tartar). This is necessary so that during orthodontic treatment you do not encounter complications of caries and gum disease. It is important to adjust home hygiene, since orthodontic treatment worsens the conditions for self-cleaning and home dental hygiene [2]. It is necessary to use the entire arsenal to clean teeth with braces: an electric toothbrush or a special manual brush for braces, interdental brushes, superfloss, irrigator). It is also recommended to carry out professional hygiene in a dental clinic once every three to four months. If ideal hygiene is not observed, carious cavities quickly form.
Treatment of deep bite in children
Correction of a deep bite occurs most quickly during the years of formation of a mixed dentition in children, that is, from the age of 7 (the time of eruption of the first permanent molar). At this age, bone tissue is softer and teeth move faster. Orthodontists help shape a physiological bite using removable orthodontic plates.
Deep bite cannot be corrected only by moving the teeth without taking into account the reason that caused it [9]. For example, if the bite is corrected and the child continues to suck the thumb, this can lead to a relapse. If a child has bruxism and increased wear of the lateral teeth, then first of all it is necessary to consult a neurologist and psychologist, since one of the causes of childhood bruxism is stress. After this, you can restore the bite height.
Treatment of deep bite in adults
Treatment of adult patients is usually carried out using orthodontic methods (braces). This technique consists of aligning the position of the teeth to distribute an even chewing load on all teeth. The treatment result is considered good if the upper incisors overlap the lower ones by 1/3 of the crown length, the shape of the dental arch of the upper jaw is semi-elliptical, and the shape of the lower jaw is parabolic. The advantages of this technique are that the maximum number of teeth remains without grinding or depulping.
The second technique is to increase the bite with the help of orthopedic structures. In this case, all teeth of the lower and upper jaw are covered with onlays/veneers/crowns. The disadvantage is that in order to install orthopedic structures, it is necessary to heavily grind off the dental tissue (for example, in the case of a roof-shaped deep bite to tilt the crowns of the upper anterior teeth inwards), which leads to the opening of the pulp. In this case, it is necessary to depulpate the teeth. This technique is not popular among dentists, but is sometimes used in practice.
The third technique is a combination of orthodontic preparation and orthopedic dental restoration. It has a number of advantages:
- Faster orthodontic treatment.
- Covering “weak” areas of teeth with orthopedic structures. Weak areas are the areas where caries most often forms (for example, between the teeth). These areas can be made of ceramic, which is similar in properties to tooth enamel, but is not susceptible to caries. Worn and chipped parts of teeth are restored with ceramic onlays/veneers.
The disadvantage of this approach is the high cost.
Orthognathic surgery
For very severe pathologies of the bite and jaw size, orthognathic surgery is sometimes indicated [5]. This is a surgical technique in which the position of the jaws is changed, their size is reduced or increased.
Before surgery, orthodontic treatment is performed. Its goal is to prepare the patient so that the post-surgical phase of orthodontic treatment can be completed within 6 months. In this case, it is necessary to align the dentition or their segments, ensuring their correspondence in size, shape and placement of the incisors. Pre-surgical orthodontic preparation takes about 12-18 months depending on the severity [5].
The operation is performed under anesthesia. The jaw is fixed in the desired position using special titanium plates. Depending on the complexity of the operation, the patient must spend 2 to 4 days in the hospital. At the end of this period, the patient's jaws are fixed in the correct position with intermaxillary traction for 6 weeks. After surgery, orthodontic treatment usually takes from 3 to 6 months [5].
The goals of orthognathic surgery coincide with the general goals of treatment:
- make a stable bite;
- distribute the chewing load evenly;
- simplify home hygiene and oral sanitation;
- eliminate dysfunction of the temporomandibular joint;
- improve aesthetics [5].
About 90% of patients who have undergone orthognathic treatment are satisfied with its result and more than 80% note that, knowing the process and result of the treatment, they would undergo it again and would recommend it to others [7].
If surgical treatment is impossible (in the presence of moderate and severe periodontitis, diseases of the temporomandibular joint in the acute period, precancerous diseases, acute and chronic low-grade inflammatory processes in the area of the planned intervention, or when the patient refuses surgery), the oral cavity is sanitized and the occlusion is stabilized in a central ratio, using orthopedic structures and special protective night guards. This help is aimed at improving the closure of teeth, however, it will not be possible to correct severe dental anomalies and improve aesthetics in this way.
Treatment of deep bite with dysfunction of the temporomandibular joint
Treatment begins with relaxation of the masticatory muscles using muscle relaxants and a bite pad. Then the central relationship of the jaws is found. This is a position of the lower jaw in which all muscle and articular structures are in a relaxed state, and the head of the joint of the lower jaw is located in the anterior-superior position of the glenoid fossa.
The next stage is fixing the jaw in centric relation using a removable mouthguard and carrying out the necessary treatment. Subsequently, the lost tooth tissue is restored using orthopedic structures: veneers, crowns or ceramic onlays.
Surgical treatment of mandibular hyperplasia.
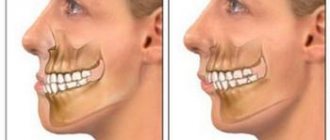
If the height of the mandible is significantly increased, facial symmetry may be improved by surgical reduction of the lower edge of the jaw. High condylectomy surgery effectively stops disproportionate jaw growth while maintaining normal jaw function. Patients with active hyperplasia are treated with high condylectomy, articular disc reduction, and orthognathic surgery. The pathogenesis is most likely related to a disorder of condylar hyperactivity, which can be documented histologically by actively proliferating cartilage. Hyperplasia of the hemimandibular, including the condyle, requires more careful treatment planning compared to these anomalies limited to the ramus and body of the mandible, which require an accurate diagnosis to ensure appropriate treatment.
Prevention methods
Parents can prevent malocclusion in their child if they take care of their oral health and visit a specialist once every six months.
Habits that should alert a parent:
- sitting, the child constantly props up the same cheek with his hand;
- often touches growing teeth with tongue or hands;
- asymmetrical arrangement of the jaws.
Sleeping on the wrong pillow can be harmful: too high or low. This leads to curvature of the spine and malocclusion.
Only a doctor can make an accurate diagnosis. If you see the listed signs in your baby, visit the Russdent clinic. Our specialists will quickly and painlessly carry out a competent diagnosis and choose a strategy for further work with the patient.
Treatment at Russdent
Our clinic employs the best doctors who have extensive experience and constantly improve their skills through training. In addition, the clinic has modern equipment, which is important for early diagnosis. We use up-to-date treatment methods that provide high effectiveness even in difficult cases. These are the American systems “Damon Q”, “Damon Clear”, “H4”, as well as the lingual systems “Win” (Germany), “Incognito” (USA). For soft correction, transparent Invisalign aligners are used.
For more detailed information, please contact the clinic for a consultation.
What can cause hypoplasia of the lower jaw?
Mandibular hypoplasia tends to be a congenital condition, however, it can definitely occur due to trauma or. Mandibular hypoplasia indicates an incomplete jaw. The radiographic appearance of maxillary and mandibular lesions often includes radiolucency with poorly defined or even irregular diffuse borders. Expansion of the orbital border usually creates hypoplasia and poor pneumatization of the ipsilateral maxilla. Possible hypoplasia of the body of the lower jaw, an abnormal coronoid process, as well as a zygomatic arch.
Problems with large teeth
Whenever we talk about a slight deviation from the norm or a slight disproportion, enlarged crowns do not entail any problems. Large front teeth are in fashion today, as they give the face a more youthful appearance, so it is not always possible to even talk about aesthetic flaws. But if we are talking about pathology, then too large teeth entail unpleasant consequences.
- Large teeth do not have enough space, which is why they can curl and extend beyond the dentition. This forms an incorrect bite and affects not only the aesthetics of the smile, but also digestion.
- A large molar in a child often causes a delay in the eruption of neighboring teeth.
- If the patient’s teeth are not large by nature, but have become so over time, this indicates gum disease. It must be cured before proceeding with the elimination of aesthetic defects.
- Teeth that are too large can distort speech.
- People with disproportionate teeth face psychological problems: they are embarrassed about their smile, try to communicate less, and feel self-conscious.
How is it diagnosed?
Pruzansky classified mandibular hypoplasia as grade 1, 2, or even 3. Class 1 refers to the small size of the lower jaw, regardless of the average configuration. Some patients were diagnosed with congenital hypoplasia of the mandible, devoid of any recognized syndrome. Diagnosis of the lower jaw includes:
- Hypoplasia of the lower jaw;
- Hyperplasia of the lower jaw;
- Hypoplasia of the lower jaw with dentoalveolar hyperplasia;
- Hyperplasia of the lower jaw with dentoalveolar hyperplasia;
- Dentoalveolar hyperplasia;
- Neonatal enamel hypoplasia associated with premature birth or possibly early febrile illness.
Significant signs are also rib rupture defects, which can contribute to rib fracture. This jaw hypoplasia occurs in children with a special focus on the respiratory tract. Mandibular hypoplasia can be classified according to the Pruzansky classification system developed in 1969. The underlying pathology is actually mandibular hypoplasia, which throughout fetal life creates an inability for the tongue to migrate caudally, causing abnormal tongue positioning and obstruction of regular palate growth.
Evolution of tooth size
Our distant ancestors, who lived about 100,000 years ago, had very large teeth - about twice as large as those of modern humans. This was a vital necessity. With the help of teeth it was necessary to gnaw animal bones and tear raw meat. But with the development of the brain and changes in diet, they gradually decreased. Scientists have calculated that every thousand years, 1% of their surface “gone” (although it is possible that over the past centuries this process has accelerated significantly).
The changes affected not only the overall size of the teeth, but also their purpose. The largest tooth in modern humans is the first upper molar: in the process of evolution, the main functional role has passed to it from the second upper molar. The fangs, which were no longer so important for holding food, were transformed the most.
How is hypoplasia of the lower jaw treated?
To lengthen the mandible in situations such as mandibular hypoplasia or post-traumatic defects of the mandible, gradual distraction of the bone tissue is required. Treatment will depend on the degree of midfacial hypoplasia as well as the structures involved. Most patients with craniofacial microsomia actually have a level of mandibular hypoplasia, which is clinically seen as a form of receding chin and asymmetry at the corners of the mouth. There is hope for those suffering from mandibular hypoplasia, but it requires a reconstructive surgical procedure. The extent of the operation depends on the level of underdevelopment, as well as on the configuration of the surrounding tissues and muscles of the face.