Dentinogenesis imperfecta type I
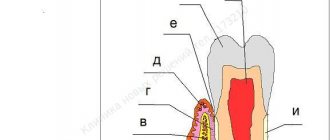
Pathology is always combined with osteogenesis imperfecta. It occurs more often in men, frequency - 1:50,000. General clinical signs may vary depending on the type of inheritance. Teeth wear out quickly and become more intensely colored, and are sometimes affected by caries. In permanent teeth, the clinical picture varies. On examination, the bulbous shape of the teeth and root fractures are noticeable.
The diagnosis is confirmed by x-ray. The image shows thinning of the cortical layer of the jaw and the coarse structure of the spongy substance. After eruption, obliteration of the roots begins, which slowly progresses.
The main pathological signs are:
- normal enamel structure;
- enamel-dentin junction in the form of a straight line;
- a decrease in the number of dentinal tubules in the peripulp dentin, their uneven diameter, narrowing and obliteration;
- deficiency of dentin mineralization;
- absence of conversion of precollagen fibers into collagen fibers.
Causes
An anomaly appears when there is a disturbance in the development of hard dental tissues. The patient develops amorphous, disorganized, atubular dentin with a high content of organic microelements. The first category of disease is characterized by a lack of collagen. In the second type of disease, the main provoking factor is a defect in the DSPP gene. The provocateur of the third type of pathology is a violation of the phosphoprotein matrix, which is part of the hard tissues of the masticatory organs. In newborns (1 case per 17.5 thousand), the disease has a hereditary factor.
The mechanism of infection can be autosomal dominant, recessive or non-mutational. The genetic risk of the lesion is 50%. To identify the cause of the anomaly and develop the correct treatment plan, it is better to contact a private dental clinic. Only qualified specialists will be able to understand this issue. Self-medication is unacceptable. After all, such heterogeneous genetic damage can combine several diseases with different etiologies, which have the same clinical picture.
Type II dentinogenesis imperfecta
This pathology is otherwise called hereditary opalescent dentin, or “crownless teeth.” It occurs with a frequency of 1:8000, develops in an autosomal dominant pattern and has another name: Stainton-Candepont syndrome. As a rule, the disease is not combined with general diseases.
The enamel turns watery gray, amber or purple-blue, and the teeth become translucent. Sometimes the crowns take on a purple hue and are shaped like an onion. 2-4 years after teething, the enamel begins to actively chip off. The occlusal surface of the teeth is characterized by increased abrasion, and exposed dentin turns brown.
Additional clinical signs include increased electrical excitability of the pulp and a possible delay in root resorption of primary teeth. In some patients, on the contrary, early replacement of milk teeth with permanent teeth is observed, and caries is rare with this pathology.
X-ray signs:
- the roots may be shortened, with hypercementosis, with foci of clearing in the apical area;
- dental cavities are reduced, the canals are narrow or obliterated, which is a consequence of progressive calcification;
- the height of the crowns is reduced due to rapid abrasion;
- There are areas of rarefaction of bone tissue in the area of the root apexes.
Pathomorphological features:
- The structure of the enamel is disrupted, the tissue becomes thinner, the number of organic plates increases, and areas of structureless enamel are noticeable.
- At the enamel-dentin junction there is a straight line.
- The structure of dentin is heterogeneous.
- The number of tubes in the peripulpar dentin is reduced; they are short, curved, expanded and grouped in several pieces.
- The amount of interglobular dentin increases.
- In dentin, the amount of mineral substances decreases (60%), while the amount of water (25%) and organic substances (15%) increases.
- Hydroxyapatite crystals are replaced by an amorphous structure.
- The dentin matrix has an atypical structure, and predentin is expanded.
- The number of odontoblasts decreases, the shape of the cell and nucleus changes, processes are absent, and in some cases the odontoblasts themselves are absent.
- The pulp has few vessels, but many denticles and fibers.
- Degenerative changes in the cement are noticeable.
Diagnostics
One of the most important stages in diagnosing this pathology is collecting an anamnesis coupled with identifying unfavorable hereditary factors. The clinical manifestations of the disease directly depend on its form.
On physical examination, a change in the shade of tooth enamel is observed. The crown takes on a spherical shape and noticeably narrows in the neck area. Additionally, severe abrasion is detected in combination with a “decrease in the lower third of the face.”
It is necessary to differentiate dentinogenesis imperfecta not only from amelogenesis imperfecta, dentin dysplasia, acid necrosis, anomalies of tooth development, but also from other pathological changes in dentin associated with a number of other, more rare diseases. In particular, it is necessary to mention brachioskeletogenital syndrome, marble disease, hypophosphatasia, and Ehlers-Danlos syndrome.
In order to identify genetic factors in the occurrence of pathology, a medical genetic consultation may be indicated.
Type III dentinogenesis imperfecta
This form is rare and is considered an isolated hereditary form of wine opalescent dentin. With it, the crowns of the teeth take on the shape of a bell. Multiple openings are noticeable in primary teeth. The x-ray shows a contrasting contour of the tooth with internal enlightenment. This is explained by the fact that after the formation of the outer covering layer, dentin production ends.
Symptoms
Symptoms largely depend on the category of pathology:
- If the patient suffers from the first form, his units erupt in time and are of normal size. But the patient complains of bleeding gums, as well as mobility of the chewing organs. Its dentin has a pronounced gray-watery color. Sometimes crowns resemble the shape of onions. A high degree of enamel abrasion and root fractures are often diagnosed.
- The second form of pathology has an isolated character. Dental tissues are stained amber or have a gray-watery tint. Less commonly, chewing organs are purple in color. Sometimes the crowns become short and have an onion-like shape. A distinctive feature is the progressive obliteration of the pulp chambers, which forms before the units erupt. If a chip appears on the crown, the dentin quickly becomes exposed, the height of the bite decreases, and the head in the temporomandibular joint shifts. Gradually, the teeth acquire a brown tint. At the same time, the roots become thinner and curved. Additional signs: high degree of electrical excitability of the pulp, delay in temporary organs of root resorption. But, in some patients, the change of milk units occurs ahead of schedule. In such a situation, caries rarely occurs.
- The third type is distinguished by the fact that the permanent masticatory organs are bell-shaped. Their color is brownish-yellowish or bluish-gray. Typically, in this situation, the pulp chambers are characterized by multiple openings.
It is useful to remineralize teeth. During fluoridation, the enamel is saturated with mineral elements. This technology restores the structure of the crown. The procedure can be artificial or natural. In the latter case, the enamel is restored due to the patient’s nutritious diet and taking vitamin and mineral complexes. With the artificial technique, the enamel is covered with protective compounds that include fluoride or mixtures without fluorides.
Treatment of dentinogenesis imperfecta
Unlike the treatment of pulpitis of baby teeth or caries, with this diagnosis, mainly orthopedic rather than therapeutic dentistry is possible. If the primary teeth are completely worn down, complete plate-type dentures are made and placed over the roots. With their help, they monitor the functional load when chewing, and also provide optimal conditions for changing the bite to a permanent one. The prosthesis also maintains the myodynamic balance of the masticatory muscles, the height of the bite at the beginning of its formation, and compensates for aesthetic defects.
If the teeth are not completely worn down, individual thin-walled stamped crowns are made to maintain the height of the bite. They also cover permanent molars and incisors that have just erupted. These actions are aimed at stopping the abrasion of hard tooth tissues and increasing the height of the bite.
Once the permanent teeth have fully erupted, the temporary crowns are replaced with permanent ones. Due to obliteration of the root canals, the manufacture of pin structures is excluded, however, parapulp pins and composite materials can be used to build up missing tissues before prosthetics.
Anatomical dental pathologies
Dental anomalies are deviations from the physiological norm in the size of teeth, their number, color, shape, structure of hard tissues, timing of eruption, position in the dentition. All these pathologies are associated with improper formation of the dentofacial apparatus and are accompanied by aesthetic defects, deformation of the maxillofacial area, malocclusion and diction, and difficulties in chewing food.
Edentia
Adentia is the partial or complete absence of teeth as a result of disruption of their formation.
If you do not seek dental help when symptoms of partial edentia are detected, the jaw will begin to deform and malocclusion will develop. The complete absence of teeth will lead to gastrointestinal diseases, poor functioning of the body as a whole and impaired quality of life.
Dystopian teeth
Teeth that are incorrectly positioned in the dental arch are called dystopic, and the anomaly of such teeth itself is called dystopia.
Displaced teeth significantly spoil the aesthetics of a smile and lead to disturbances in the functioning of the maxillofacial area, the masticatory apparatus and complications: the occurrence of caries, periodontitis, ulcers on the oral mucosa, inflammation of the soft tissues around the erupted tooth.
Impacted teeth
Tooth retention is a delay in the eruption of a fully formed dental unit.
An impacted tooth contributes to the development of dental defects, chronic gum diseases, and the appearance of cysts. In this regard, retention requires mandatory orthodontic and surgical treatment.
Hyperdontia
Hyperdontia (polyodontia) is an anatomical anomaly manifested in the presence of supernumerary teeth.
Supernumerary teeth cause various anomalies of the dental system and inflammatory-dystrophic changes in the surrounding tissues. Often due to hyperdontia, malocclusion is formed, speech defects appear, and the eruption of permanent teeth is delayed.
Microdentia
Microdentia is an anomaly in which the teeth are significantly smaller than their anatomically normal size.
Pathologically small teeth differ from anatomically normal ones by at least 1.5 mm in both diameter and height. Because of this, gaps form between the teeth, which can subsequently lead to periodontal tissue diseases.
Macrodentia
Macrodentia is an anomaly of teeth in which their crown part is significantly larger than the anatomically normal size.
Disproportionately large teeth contribute to deformation of the bones of the facial part of the skull and malocclusion. The person experiences psychological discomfort. The consequences of macrodentia can be successfully eliminated using modern orthodontic methods.
Amelogenesis imperfecta and dentinogenesis
Amelogenesis imperfecta is a rare hereditary anomaly of enamel formation, which manifests itself already at the stage of intrauterine development. The disease usually accompanies dentinogenesis, a genetic pathology of dentin formation.
If teeth affected by imperfect amelo- and dentinogenesis are affected by caries, it will begin to spread quickly, since the enamel and dentin layers are weakly connected.
Treatment of dental fluorosis in children
Treatment methods depend on how far the process of destruction of the enamel or the tooth itself has progressed.
- For streaked and spotted forms of fluorosis, dentists use microabrasion and remineralizing therapy of tooth enamel.
- If the integrity of the enamel is noticeably damaged, the surface is restored by filling and/or microprosthetics.
- In case of erosive and destructive forms (deep damage to dental tissues), it is necessary to use metal and ceramic crowns, as well as structures to fix the remaining part of the tooth.
Provoking factors
Since dentinogenesis imperfecta is a hereditary disease, gene mutations that manifest themselves at the stage of bone formation, blood vessels and dentin formation in the fetus act as provoking factors.
The role of other risk factors for the development of pathology is unclear. However, it is obvious that the general state of health, immune status, quality of nutrition and oral care, injuries, and lack of planned sanitation of the oral cavity have a negative impact on the development and severity of the disease.
Therefore, the role of preventive measures against any dental diseases remains important in this case.
Dental hypoplasia in children: causes
Hypoplasia of primary teeth in children often develops due to the condition of the mother during pregnancy and disruptions in the process of formation of tooth buds in the fetus. Particularly dangerous are diseases such as toxoplasmosis, rubella, severe forms of toxicosis, and Rhesus conflict. Prematurity and illnesses suffered immediately after birth can also subsequently cause systemic enamel hypoplasia.
A special cause of severe systemic hypoplasia is the use of the antibiotic tetracycline by a woman during pregnancy or by a child in infancy. In this case, the teeth darken, the enamel is destroyed, and sometimes it may be completely absent (enamel aplasia).
Hypoplasia of permanent teeth in children develops due to diseases suffered at the age of 6-18 months, when the rudiments of future teeth are formed:
- Severe ARVI;
- Intestinal infections;
- Digestive pathologies;
- Vitamin D deficiency, rickets;
- Dystrophy, lack of nutrients.
Diagnostic measures
Diagnosis of dentinogenesis imperfecta involves both standard diagnostic dental procedures (examination of the oral cavity and radiography) and special ones, such as clinical and genealogical research aimed at identifying hereditary dental diseases and their characteristics.
With the help of an examination, the color and shape of the crown part, the presence of stains on it, and the degree of abrasion of the teeth are determined. In particular, the spherical shape of the crown may indicate imperfect dentinogenesis.
Based on radiographs, the condition of the root part of the tooth is determined (presence of canal obliteration, bone resorption) and the thickness of the walls of the pulp chamber.
When conducting a hereditary genealogical examination, a pedigree of family members is compiled (preferably no less than 3-4 generations) and the presence of genetically determined diseases of the jaw apparatus is determined.
The data obtained serve to clarify the diagnosis and make a prognosis for the offspring.
Characteristics of Pulposeptin paste and instructions for use in dentistry in the treatment of gangrenous pulpitis.
In this publication we will talk about the pathology called “Turner’s teeth”.
Here https://www.vash-dentist.ru/lechenie/zubyi/ultrazvuka-v-endodontii.html all about the benefits of ultrasonic expansion of the root canal of a tooth.
Classification
Since amelogenesis imperfecta belongs to a genetically and clinically heterogeneous group, its classification was not easy to create. The first systematization was based on phenotype and had 2 types of disease. Then scientists identified 5 groups of pathology, and later presented four main types, which were based on phenotype, as well as inheritance. The comprehensive latest systematization takes into account the type of inheritance, molecular defect, phenotype, and biochemical analysis. The occurrence of the form of AN depends on the disturbances that occur in the enamel matrix.
Hypoplastic
The genetic type of this disease is the main one. It is characterized by the correct stage of formation of the enamel layer. But he's not thick enough. The affected areas are often on the surface of the buccal areas. Oval depressions or pits of varying depths, as well as grooves of varying lengths, are clearly visible. The layer is quite hard. Its surface can be rough, smooth, or granular. Healthy areas retain their shine. The depth of the defects affects the color intensity. With deep lesions, dentin is exposed.
Hypomaturation
With this form, the enamel has normal thickness, despite problems in matrix maturation. But the layer quickly becomes insufficiently hard, and the surfaces of the crowns lose their shine.
Hypomineralized
Qualitative changes occur when the matrix is mineralized. This is a rare group of pathologies that is detected in 3 percent of patients. After the eruption of the chewing organs, the thickness of the enamel is normal, the surface of the crowns is smooth.
Hypomaturation with taurodontism and hypoplasia
With such a defect, a failure occurs during tissue differentiation, as well as during the layering of the enamel matrix.
For any form of anomaly, patients should use the services of a dental clinic. Only a modern clinic with advanced equipment will help the patient get rid of the problem. The sooner you see a doctor, the easier the treatment will be, the faster the recovery period will end.
Prevention
The percentage of the disease is higher among patients with acute osteogenesis, when there is a qualitative and quantitative collagen deficiency. Specific methods for preventing pathology have not yet been developed. For prevention purposes, you should carefully observe oral hygiene rules and undergo routine dental examinations. It is necessary to carry out sanitation of the oral cavity in a timely manner. It is necessary to visit the dentist at least once every six months in order to identify the disease in the early stages, as well as to begin treatment of the pathology in a timely manner. If necessary, consult a geneticist.
Reviews
Dentinogenesis imperfecta is a relatively rare, but in some of its forms, a serious disease that must be identified and treated without delay.
Moreover, in many families, due to the hereditary nature of the disease, it is not a surprise. If you or your children have been treated for dentinogenesis incomplete, please share your personal experience about this rather rare disease. You can leave a comment at the bottom of this page.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags: enamel destruction
Did you like the article? stay tuned
Previous article
The Korkhaus apparatus as the best solution in orthodontics for eliminating diastemas
Next article
Suturing the tooth socket is a simple and safe way to restore the alveolar process after extraction