Kinds
There are several types of occlusion anomalies; in pediatric orthodontics, there are six.
The following types are distinguished:
- deep – it is characterized by excessive overlap of the upper jaw of the lower jaw;
- cross - with this violation of closure, there is underdevelopment of the jaws on one side, with a characteristic intersection of the lower and upper dental arches;
- mesial - it is typical for the lower jaw to move forward, with the lower incisors overlapping the upper ones;
- open - with this disorder there is no closure of the upper and lower incisors, the patient has a gap between them;
- distal - with this anomaly, the upper incisors move forward, this sign is combined with underdevelopment of the lower jaw and a reduction in the lower part of the face;
- underestimated - characterized by underestimated closure, due to premature abrasion of teeth.
Before starting correction, it is necessary to establish the type of occlusion violation.
X-ray safety
There is often a belief among patients and parents that dental x-rays, and in particular, children’s panoramic dental photographs, are harmful to health and “unnecessarily expose them to radiation.”
Of course, you shouldn’t do an X-ray thoughtlessly and without the appropriate doctor’s testimony. Ionizing radiation affects the body, but only in large doses.
When X-rays are taken for children at NovaDent, the amount of radiation is strictly dosed and does not exceed the permissible level, so you don’t have to worry about the health safety of the procedure.
Contact NovaDent pediatric dentistry for a consultation. Prices for x-rays in our clinic are quite affordable and start from 450 rubles.
Expert of the article you are reading: Lapshina Maria Aleksandrovna Dentist, pediatrician
21 years
Clinical experience
Krasnogorsk
Moscow region, Krasnogorsk, Podmoskovny Boulevard, 5
+7
Free consultation with this specialist
Reasons for development
Why does a child develop malocclusion? The causes of its occurrence are divided into congenital and acquired.
Causes of congenital malocclusion:
- infections affecting the fetus;
- maternal diseases complicating the development of the fetus;
- maternal abdominal injuries;
- negative effects of poisons and drugs;
- trauma to the baby's facial bones during childbirth;
- congenital shortening of the frenulum of the tongue and lips.
Unlike congenital ones, acquired closure disorders are caused by diseases and bad habits.
These reasons include:
- pacifier abuse;
- the baby constantly sucks and chews objects (pencil, finger);
- bad habits (biting your lip, propping up your chin);
- lack of prosthetics, teeth falling out prematurely;
- Consequences of rickets before the age of one year;
- pathologies of ENT organs, with impaired nasal breathing (deformation of the nasal septum, enlarged adenoids);
- endocrinopathies;
- diseases of the musculoskeletal system;
- pathological posture in sleep;
- extensive caries of molars;
- injuries to the facial part of the skull;
- malignant tumors of the facial bones;
- purulent-necrotic processes of the jaws (osteomyelitis, periostitis);
- early or delayed eruption of teeth.
Often the formation of closure defects is caused by several reasons. They need to be identified in order to determine the optimal tactics for correcting the defect.
What is being researched and why?
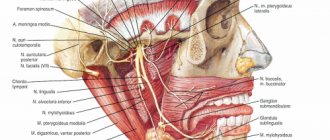
Important! An X-ray of the child’s head is performed to assess the condition of the skull, that is, the bone structures, rather than the brain.
X-rays pass differently through different organs and tissues, the images of which in the pictures, due to this, differ in intensity. So, the bone - the hardest tissue - will be bright white, and the soft structures will be gray or almost black. An overview image shows a general image of different structures of the skull: the sella turcica, eye sockets, lower jaw, temporomandibular joint, etc. To clarify the diagnosis or a detailed examination of the pathology, you need to do a targeted study (the tube of the device is directed to a specific area of the skull).
What can you find?
Radiography allows you to see:
- congenital pathologies;
- birth injuries and deformities;
- cysts;
- osteoporosis;
- hematomas;
- neoplasms;
- hernias;
- fractures;
- consequences of inflammatory diseases;
- bone condition.
How to suspect the development of a defect
How to identify malocclusion in a baby. Even a non-specialist can suspect the formation of this problem.
We list the most characteristic signs:
- uneven dental arches;
- crowding of teeth and their rotation around their axis;
- growth of units in the wrong place;
- gaps between teeth;
- presence of extra units;
- excessive overlap of the upper or lower jaw arches;
- no closure of incisors;
- facial asymmetry;
- moving one of the jaws forward;
- constantly open mouth;
- difficulty in nasal breathing;
- pathological abrasion of teeth;
- traces of injuries on the inner surface of the lips, tongue, cheeks;
- increased tone of facial muscles;
- difficulty chewing food;
- difficulty producing sounds.
Having discovered one or more of the listed signs in their baby, parents should take him to an orthodontist as soon as possible.
Photo of baby teeth
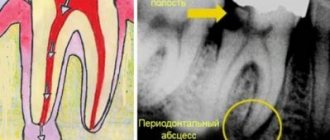
X-ray of primary teeth is an effective method to identify emerging problems.
through modern diagnostics.
As you know, many children have a hard time going to the dentist. Parents and doctors have to come up with various tricks in order to put the child in a chair and carry out the necessary procedures.
In addition, a pediatric dentist must have certain knowledge in the field of education and psychology, as well as have extensive work experience in order to know what approaches can be applied to a child for successful treatment. Not all clinics have such doctors, and the wrong approach can harm the child’s psyche and initially spoil his attitude towards the doctor’s office.
In order to prevent the need for frequent visits to the dentist, it is necessary to bring your child for preventive examinations.
An X-ray of baby teeth in children will allow you to see:
- condition of tooth roots;
- condition of soft tissues (and gums);
- determine the location of dental root primordia;
- more accurate timing of loss of primary teeth.
Since the process of replacing baby teeth with permanent ones accompanies the child and his parents for several years, it is worth paying special attention to diagnosing the position of the teeth and their quality condition.
At what age is it better to carry out correction?
At what age can you start correcting your bite in children?
It is impossible to determine malocclusion in a 1-year-old child. It is possible to suspect it if your parents have it. Malocclusion in a child from 2 years to 3 years of age can be corrected only with the help of preventive measures.
These include:
- breastfeeding up to one year;
- timely introduction of hard foods into the diet;
- use of orthodontic pacifiers;
- monitor the baby’s posture during sleep;
- promptly treat caries of primary teeth;
- if they are lost early, prosthetics are necessary.
The baby needs to be treated for somatic diseases that can disrupt the development of the dental system.
At what age is the bite corrected in children? Active correction begins in the age range from 3 to 5 years.
The following activities are carried out:
- stopping bad habits;
- use of vestibular shields;
- facial myogymnastics;
- In case of early tooth loss, prosthetics are performed.
At the age of five, plastic surgery of the short frenulum of the tongue and lips is performed.
At the age of 7 years and older until adolescence, correction is carried out with various devices for removable correction.
These include:
- orthodontic plate devices;
- trainers;
- mouth guards;
- extraoral devices.
Starting from adolescence of 12–13 years, the defect is corrected using various models of brace systems.
In adolescents over the age of 16, veneers and crowns are used to correct minor cosmetic defects in the smile area.
How to correct a child’s bite and what correction methods to use is decided only by the orthodontist.
Features of baby teeth
The structure of baby teeth is similar to permanent teeth: in the jaw there are such types of teeth as incisors, canines, premolars and molars - all like in adults. Only their number differs: for children – 20, for adults – 32.
Baby teeth are formed in the sixth week while still in the womb. After the birth of a child, teeth erupt at about 6 months and grow in by 3-4 years. The exact age depends on the individual's rate of development.
However, there are some differences from permanent teeth:
- baby teeth have long roots that are easily absorbed over time
- greater distance between teeth - so that falling out for replacement is easy
- thinner and more delicate enamel
- softer dentin and surrounding tissues
Defect correction
Correction is carried out using conservative and surgical methods.
Conservative therapy
For hardware correction, removable and non-removable correction devices are used.
These include the following devices:
For correction use:
- vestibular shields - used to wean the baby from sucking fingers and other objects;
- Trainers are used to correct minor anomalies and align the positions of individual units in the dental arch;
- correction plates are plates made of plastic and metal, used to correct anomalies during tooth replacement, they are self-regulating devices;
- aligners are silicone molds made of silicone that give a physiological bend to the dental arch.
- braces are a non-removable orthodontic structure for correcting the most complex dental defects and anomalies;
- extraoral devices – used to correct severe anomalies when braces cannot be installed.
Devices for correcting malocclusion and the position of individual teeth are selected based on the severity of the defect and age. Is it possible to correct the bite using only conservative methods? In most cases, the use of these devices is sufficient.
Surgical treatment
I use surgical techniques only in the most difficult situations, when the use of conservative methods has not eliminated the defect. They are used only in adolescence and in adults only in cases of serious deformities of the facial skeleton.
Indications for this are:
- gross facial asymmetry;
- gross anomalies of occlusion;
- underdevelopment of the chin.
After the operation, long-term rehabilitation is carried out for at least five months.
Complications
If anomalies are not corrected, then not only the baby’s appearance suffers. The consequences of impaired occlusion are numerous somatic pathologies.
What does the anomaly affect:
- diseases of the digestive tract develop;
- widespread caries;
- formation of dental plaque;
- inflammatory processes in the oral cavity;
- poor posture;
- respiratory disorders;
- disruption of the process of chewing food;
- previous tooth loss.
The baby develops articulation disorders, and the pronunciation of sounds suffers.
Prevention
Prevention of disorders begins as early as a one-year-old child. It is necessary to ensure that the baby does not suck a finger or other foreign objects so that proper closure is formed. Only orthodontic pacifiers should be used.
For an older child, preventive measures include:
- treatment of carious lesions;
- prosthetics of teeth lost prematurely;
- prevention of the development of rickets.
It is necessary to take your child for examination to an orthodontist in a timely manner in order to promptly identify closure disorders and resolve the issue of correcting it.
Violation of occlusion is a defect that threatens not only cosmetic defects, but also the development of a large number of serious diseases. Parents should, if they have the slightest suspicion of the development of this anomaly, take their child for examination to an orthodontist.
Types of X-rays of children's teeth
- Sight shot
- allows you to “enlighten” one or two adjacent teeth and see its detailed condition, as well as the condition of the surrounding soft tissues.
- Panoramic shot
(or, in other words, orthopantomogram) - displays a complete picture of the jaw and dentition, allows you to see not only baby teeth, but also all the rudiments of permanent ones. A panoramic photograph of a child’s teeth is taken during the period of active eruption of permanent teeth or before the start of orthodontic treatment.