Purulent nasal discharge can appear for many reasons and necessarily require treatment. You should not carry out therapy on your own due to the risk of severe complications if treated incorrectly. As soon as purulent discharge from the nose is noticed, you should immediately seek medical help from an otolaryngologist, or, in his absence, a therapist. The fact that pus, and not ordinary snot, began to come out of the nose can be understood by a special, extremely unpleasant odor, which does not occur with a simple runny nose. The yellow-green color of the discharge also differs from the usual one.
The appearance of pus from the nose can be associated with a number of diseases. In order to effectively treat a problem, it is necessary to accurately determine the reason why it occurs. If you seek medical help in a timely manner, the therapy quickly produces positive results and nasal discharge disappears. If for some reason the disease turns out to be advanced, then treatment may take a long time and sometimes require surgical intervention. The appearance of pus from the nose occurs equally in adults and children and requires similar therapy. It is not uncommon for purulent nasal discharge to appear after viral infections as a complication of the disease. In order to prevent this phenomenon, it is necessary to fully treat the primary disease without suffering it on your feet.
When the pus is liquid and white, this is an indicator of the initial stage of the disease. In this case, it is released in large quantities, and also often flows down the back wall of the pharynx. If the particles of pus are viscous and more like lumps, then this is an indicator of severe neglect of the purulent process. Most often, with long-term disturbance, green nasal discharge occurs. The formation of pus is always associated with the penetration of pathogenic bacteria into the nasal cavity. If they are absent, then a purulent process cannot occur. Because of this, in the viral form of rhinitis, the appearance of pus always indicates a secondary bacterial infection.
Compound
Pus contains:
- purulent “serum” (lat. liquor puris) - a liquid with a high content of albumins, globulins, proteolytic, glycolytic and lipolytic enzymes of microbial or leukocyte origin, cholesterol, lecithin, fats, soap, DNA impurities, histolysis products, sometimes (with purulent catarrhal inflammation ) - mucus; fibrin is usually absent, as a result of which the pus never coagulates (fibrin can appear due to mixing of pus with blood or the absence of proteolytic enzymes in the pus).
- tissue detritus;
- cells, mainly living or degenerated microorganisms or neutrophilic leukocytes (“purulent bodies”, balls, cells). In some cases, eosinophils or mononuclear cells predominate in the pus; lymphocytes or epithelial cells may also be present (with catarrhal inflammation).
In a calm state (in body cavities, in vitro), pus is divided into two layers: the lower layer is cloudy, thick, rich in clinin elements and detritus, and the upper layer is liquid and transparent. Sometimes this settling is so significant that the upper liquid layer is no different from serous exudate or even transudate (this can lead to diagnostic errors, for example. - During puncture).
Why gums fester: reasons
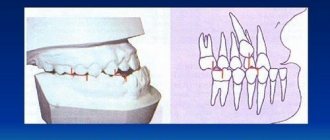
1) With an exacerbation of chronic periodontitis , infection in the root canals leads to the formation of a focus of purulent inflammation at the apex of the tooth root. Depending on the type and size of such lesions, dentists call them by terms: granuloma, cyst or granulating periodontitis. You may not be aware of the presence of such foci for years, but sooner or later an exacerbation of chronic inflammation occurs, and then pus-filled abscesses form in the projection of these foci on the gums (Fig. 1-2).
2) Against the background of inflammation of the gums (with periodontitis) - in slightly less than half of all cases when the patient's gums near the tooth fester - the cause is a local or generalized form of periodontitis. Despite the fact that the causes of these two forms of periodontitis are different, the common thing is that the formation of a purulent abscess occurs in a deep periodontal pocket formed between the gum and the surface of the tooth root. Below you can see what an abscess on the gum looks like during periodontitis (Fig. 3).
The causes and treatment of an abscess on the gum will always be interconnected, and therefore, depending on the background of what disease (periodontitis or periodontitis) the suppuration occurred, either treatment of the root canals and the source of inflammation at the apex of the tooth root will be indicated, or treatment of the periodontal pocket using anti-inflammatory therapy , curettage and other methods. Below we will discuss in detail the treatment of gum suppuration in both cases.
Properties
Pus is alkaline; when fatty and other acids are formed in it, the reaction can become neutral or acidic. The specific gravity of pus ranges from 1.020 to 1.040. Serum consists of 913.7 parts of water, 78.57 parts of organic and 7.73 parts of inorganic compounds, that is, close to blood serum.
The pus in the body cavity, without “finding a way out” for a long time, undergoes significant changes: purulent bodies and other cells disintegrate into fine-grained detritus (partly protein, partly fatty), while the liquid part is only slightly absorbed, which is explained by the presence of a pyogenic membrane around the accumulations of pus, and partly by compression of the draining lymphatic tracts.. Proteins disintegrate and can become the basis for the formation of cholesterol crystals. Bacteria in old pus also undergo dissolution, probably due to the isolation of purulent accumulations and the weak ability to renew nutrient substrates; sometimes in old abscesses changes in the cultural and biological properties of bacteria are observed, for example. — Reducing their virulence.
Purulent bodies contain glycogen, during prolonged suppuration, and droplets of fat, which often gives the pus and the walls of the ulcers a clear yellow tint. In purulent bodies, the existence of proteids (the “hyaline” substance Rovida) has also been proven, which determines the ability of pus in a solution of table salt to sometimes turn into a mucus-like mass: this is why (for example, in the bladder with cystitis) pus can undergo transformation into mucus.
The consistency of the pus is liquid or more or less thick, sometimes creamy or mucous. At the beginning of suppuration, as a rule, the pus is rare and quite transparent (seropurulent leakage). Later it becomes cloudy and thick. Thick pus, as a rule, forms at the end of suppuration, which is where the old aphorism “pus bonum et laudabile” comes from, which indicates the successful excretion of the so-called. materia peccans and emphasizes the favorable prognosis of the process. Thickening of pus is evidence of a decrease in exudative phenomena and the beginning of restoration (for example, granulation) processes.
The color of the pus is often yellow, yellow-green, or white-yellow, but can be blue, bright green, or dirty gray. The color of pus is due to the specific characteristics of the microorganisms that lead to its formation. Thus, the green color of pus is due to the presence of myeloperoxidase, an intensely green antimicrobial protein produced by certain types of leukocytes. The blue color of pus is usually caused by Pseudomonas aeruginosa due to the pigment pyocyanin that it produces. The brown color of pus is characteristic of amoebic suppuration. The reddish tint of pus forms when it mixes with blood or due to streptococcal infections.
The smell of pus is usually strong and specific, but with putrefactive (ichorous) inflammation it takes on the character of “they.” The color, consistency and smell of pus are very variable, they depend on the location of the inflammation, the type of tissue affected, the combination of the abscess cavity with hollow organs, and the nature of the pathogen.
Exacerbation of periodontitis
Cause and mechanism of development
Periodontitis is an inflammatory disease associated with infection in the bone at the apex of the tooth root. Infection can enter the bone in different ways: through a tooth root canal or through a periodontal pocket.
- In the first case, the development of the disease begins with caries. If caries is not cured in time, the infection spreads deep into the tooth and causes pulpitis, and if further untreated, microorganisms spread deeper along the neurovascular bundle inside the tooth and reaches the bone.
- In the second case, the cause of infection in the bone is a problem in the interdental space (deep pocket). Inflammation of the gums can begin due to the accumulation of tartar, due to chronic injury from the sharp edge of a crown or filling, due to improper position of the tooth in the arch, and for many other reasons. Gradually, inflammation from the gums spreads to the circular ligament of the tooth, the ligament is destroyed, allowing microbes access to the space between the tooth root and the alveolar bone.
In both cases, the entry of microbes into the bone is accompanied by the release of a large amount of toxins, the bone begins to deteriorate, and in its place a cavity filled with pus forms. The process can go relatively unnoticed, causing inconvenience to the patient only during periods of exacerbation against the background of acute respiratory infections or other conditions accompanied by a general decrease in immunity.
Gradually accumulating, the pus continues to dissolve the bone, causing the inflammation to become larger. At the moment when the amount of pus reaches a critical level (or, due to a decrease in immunity, it becomes more), the pus begins to look for a way out. The bone gradually dissolves, passages are formed through which pus comes out under the periosteum and at some point a breakthrough occurs. Through this fistula, the pus comes out, and the original process returns to its chronic course.
Symptoms
Outside of periods of exacerbation, manifestations of periodontitis are minimal. This may be discomfort when biting on a tooth, or when pressing on the gum in the area of the causative tooth, but there are no other manifestations.
During the period of exacerbation, the following symptoms occur:
- acute pain when biting on a tooth (before an abscess appears on the gum), and after the fistula opens and the pus flows out, the pain goes away;
- the feeling of a grown tooth (also goes away after opening the fistula);
- pain and swelling of the gums in the area of the causative tooth;
- A whitish bubble appears on the gum, filled with liquid contents, when opened, pus flows out.
Symptoms of general intoxication may occur: fever, general weakness, lethargy, headache.
Diagnosis and treatment
To make an accurate diagnosis, they collect anamnesis, examine the oral cavity and the possible causative tooth, and be sure to take an x-ray.
The x-ray will show dark areas in the bone that are located in the area of the tooth root. The size of these lesions can vary from a few millimeters to a centimeter in diameter or more. Most often, an x-ray can tell you exactly where the source of infection is located, on which root (or between the roots of the teeth). The image determines the condition of the bone, the condition of the causative tooth and a possible prognosis for the future life of the tooth. Based on these data, a decision is made on the treatment method.
Possible treatment options for periodontitis in the acute stage
- Therapeutic treatment. This method involves removing nerve remnants from the canals (or unsealing them if the tooth has previously been treated), antiseptic treatment of the root canals, introducing medicinal drugs into the canal, and after some time (from a week to several months) the canals in the tooth are permanently sealed . It is assumed that with this treatment the source of infection will be removed (more than 90% of microorganisms responsible for the development of periodontitis live not in the bone itself, but in the root canal system, so high-quality canal treatment often leads to complete victory over the infection and restoration of the bone). After time (six months to a year), the bone is completely restored, and the gums heal with the formation of an invisible scar. To speed up the healing of the fistula tract, it is sometimes washed with a weak antiseptic solution or cleaned with ultrasound.
- Surgical treatment with tooth preservation. There are several options for this operation. If the inflammation is at the apex of the root, then the apex of the root is removed (the operation is called “resection of the apex of the tooth root”) and the cavity in the bone is cleaned. This method assumes that the canals are well sealed, at least 2/3 of their length. The second option is to remove half the tooth (hemisection operation). This type of operation is performed on multi-rooted teeth if inflammation is observed on one root, and the second root does not have such problems. The third option (when there is inflammation between the roots in a multi-rooted tooth) - the tooth is left unchanged, and only the bone between the roots of the tooth is cleaned. All these methods assume that the inflammation came from the tooth, and not through the periodontal pocket (since if the infection came through the pocket, then after the intervention the cavity will soon be populated with microbes again, and the inflammation will progress further). For each of these operations there are certain conditions, the observance of which is mandatory for a favorable prognosis. Thus, resection is carried out only if the canal is well sealed, at least 2/3 of the length, hemisection also implies that the root that remains in the bone will be well treated, and cleaning between the roots is carried out only if all canals are well sealed.
- A combination of therapeutic and surgical treatment. If the tooth has not been previously treated (or has been treated, but the canals are poorly sealed), then before undergoing any of the above operations, the tooth must be prepared. Therefore, the canals are treated first, and only then surgical intervention is performed.
- Removal of a tooth. If the focus of destruction in the bone is large (for each patient and for different teeth the concept of “large” will also be different), if the infection came through the periodontal pocket, if the tooth is not valuable for further prosthetics, the canals in it are impassable, there are cracks and there are other - conditions due to which the tooth cannot (or is impractical) to be saved, such a tooth is removed. You need to understand that sometimes doctors leave something that, by and large, would need to be removed, and sometimes, on the contrary, they remove a tooth that could still be fought for. As an example: they leave mobile teeth in elderly people, since they are the only ones that hold a removable denture, or they remove a tooth with inflammation between the roots in a young patient in order to preserve bone volume for future implantation. In any doubtful case (when you can try to treat it, or you can immediately remove it), they focus on a further prosthetic plan. If implantation is planned, it is better to remove all questionable teeth, and if bridges or removable dentures are used, they try to fight for every tooth.
You can read more about treatment and operations in the article about jaw cysts.
Microorganisms
Microorganisms are almost always found in pus, which are the cause of its formation. The formation of pus is often caused by pyogenic bacteria (staphylococci, streptococci, gonococci, meningococci, E. coli, Proteus, Klebsiella, pseudomonas, as well as putrefactive anaerobic clostridia (Cl. Perfringens, Cl. Sporogenes, Cl. Putrificum, etc.). The formation of pus is also observed with the development of inflammation caused by other microbes (salmonella, shigella, brucella, pneumococci, mycobacteria) or fungi (candida, actinomycetes, etc.).Sometimes in the pus of microorganisms it is not possible to detect it, which may be due to the lysis of bacteria or a non-microbial cause of inflammation (such turpentine, croton oil, digitoxin, calomel, kerosene and other substances can cause suppuration).
What diagnoses can fall into the category of “abscess on the gums”?
- Exacerbation of chronic periodontitis;
- Exacerbation of chronic gingivitis (periodontitis).
Suppuration also occurs after tooth extraction (alveolitis), with cancer, with fractures (osteomyelitis) - these conditions are also accompanied by the release of pus, but here the patient (in most cases) knows about the cause (a tooth was recently removed, there was a fracture, etc.). d.). Sometimes manifestations of diseases of the mucous membranes are confused with ulcers - aphthous stomatitis, herpetic stomatitis and others, which also appear as a white (white-yellow/gray) area of the mucous membrane with a red rim around, but as such there is no pus there, and the causes of these conditions are also different. Therefore, we will talk more about periodontitis and periodontitis.
study
Pus, like all exudates, is subject to mandatory microbiological examination. In case of closed (from the external environment) suppurations, it must be taken by puncture, to the opening of the lesion, in open processes - from the depths of the focus. Examination of pus should be carried out immediately after collection to avoid lysis of bacteria. Preparations from pus are examined microscopically after staining them with Gram or other special methods. Sowing is carried out quantitatively on simple and blood agar, less often - on special media (ZhSA, Levin, with furagin, etc.)
Diagnostics
Purulent vaginal discharge with an unpleasant odor is a serious reason to contact an obstetrician-gynecologist to find out the causes of suppuration. The examination of patients involves a physical and instrumental examination of the genitals, various laboratory methods aimed at clarifying the etiological factor. The following have the greatest diagnostic value:
- Gynecological examination
. To obtain a complete picture of the disease, examination of patients with purulent leucorrhoea is carried out without preliminary preparation and toileting of the external genitalia. When examined in speculums, accumulations of thick pus can be detected on the walls of the vagina; hyperemia and swelling of the mucous membrane are typical. - Ultrasonography
. Ultrasound of the pelvic organs allows you to find out the reasons associated with purulent vaginal discharge. During standard or transvaginal sonography, the condition of the genital organs is assessed, the accumulation of hypoechoic fluid in the uterine cavity is detected, and signs of an inflammatory process are detected. - Endoscopic methods
. To determine the cause of scanty purulent discharge streaked with blood, colposcopy is necessary for a targeted examination of the cervix and cervical canal. The method helps to identify erosive changes and areas of tissue atypia. - Bacteriological method
. In order to identify the causative agent of a gynecological infection, microscopy of a vaginal smear is performed after staining, then the secretions are cultured on nutrient media. Modern methods - ELISA, RSK, PCR - are intended for rapid diagnosis of the cause of suppuration.
To identify laboratory signs of inflammation, general and biochemical blood tests are done. Serological tests help confirm the etiological factor of vaginal leucorrhoea with a pungent putrid odor. To exclude lesions of other pelvic organs, CT or MRI of the pelvic cavity is used. Diagnostic laparoscopy is prescribed if it is impossible to determine the causes of purulent discharge using other methods.
A vaginal smear examination is carried out to identify the causative agent of infection.
Education
Pus is formed as a result of the accumulation of a large number of leukocytes in a certain area of the human body in response to the penetration of bacterial infection agents into the tissue. The main role in its formation is played by neutrophil leukocytes - the most common type of leukocytes in human blood (40% - 75% of all leukocytes), which are formed in the bone marrow and constantly enter the blood. In response to microbes entering the sterile (normal) tissues of the body, neutrophils begin to actively move to the site of the infectious process. This active migration of leukocytes to the site of inflammation is called "chemotaxis" and is caused by specific cytokine proteins that are released by macrophages - white blood cells that phagocytize (engulf and digest) cell debris and pathogens, and also stimulate lymphocytes and other immune cells to respond to the invading pathogen. Consequently, neutrophils, when destroyed, kill bacteria, resulting in the release of chemicals that destroy bacteria (mediators of inflammation, and also cause dilation of blood vessels (inflammation) and attract even more leukocytes to “fight" the infection. In turn, neutrophils die and are phagocytosed macrophages, stimulating the formation of new active neutrophils to fight infection.Actually dead neutrophils (“purulent bodies”) form the viscous part of the pus.
Inflammation and the formation of pus is a normal protective reaction of the body to the invasion of infection. Claudius Galen (Greek Γαληνός, Latin Claudius Galenus), an ancient physician and surgeon in the school of gladiators (130-200 AD) argued that the appearance of pus in a wound inflicted by gladiators is a harbinger of healing (Pus bonum et laudabile) However, the formation of pus always indicates a threatening course of the disease or neglected filling and poses a threat to human life and health.
An example of diseases accompanied by the formation of pus is an abscess, phlegmon, boil, empyema, etc. Today, more than 54 diseases are known that are accompanied by the formation of pus
Gingivitis and periodontitis
Cause
Gingivitis is an inflammation of the gums, and periodontitis is a more severe form of the disease when not only the gums, but also the jaw bone are involved in the inflammatory process. Both diseases are often chronic and do not cause the patient much discomfort, but during periods of exacerbation more severe symptoms appear and the patient consults a doctor.
There are many causes of gum inflammation:
- hard and soft dental deposits;
- sharp edges of crowns and fillings, which constantly injure the mucous membrane;
- improperly restored contact points between teeth (due to which food accumulates in the gap, puts pressure on the gums and is an excellent place for microorganisms to settle);
- malocclusion (crowding of teeth, incorrect position in the arch);
- general diseases (diabetes, vascular problems, infectious diseases and others) can cause gum inflammation;
- changes in hormonal levels (during pregnancy, for example).
These are not all possible causes of gum disease, but most patient visits have one (or several) of these factors predisposing to inflammation in the gums.
Constant trauma (from food, the edge of a crown, tartar), microbial toxins, and impaired blood flow in the gums lead to the development of an inflammatory process. Usually, pus as such is not visible, but during periods of exacerbation, noticeable suppuration often occurs from periodontal pockets or its accumulation in the thickness of the mucosa (this formation is called a periodontal abscess).
Symptoms of gingivitis (periodontitis) in the acute stage
Patients with this diagnosis complain of:
- pain in the gums near a group of teeth;
- redness of the gums, swelling, pain when touched;
- it hurts to brush your teeth and eat;
- pus (sometimes with bloody veins) is released from the periodontal pocket or from the fistula tract (a fistula can form if the pockets are very deep);
- with gingivitis, the teeth usually do not suffer, but with periodontitis, tooth mobility, exposure of roots, pain from cold and sweet foods may be observed (since the root is more sensitive to irritants than the crown part of the tooth);
- Sometimes there is a deterioration in general health: fever, weakness, headache.
Exacerbations most often occur against the background of a general decrease in immunity (with acute respiratory infections or other diseases). In addition, periodontitis is characterized by seasonality (in spring and autumn, exacerbations occur more often).
Diagnostics
How to distinguish periodontitis from periodontitis? Outwardly, both cases may look the same: swollen gums, redness, a fistulous tract from which pus is released. In both cases, it hurts to bite on the teeth. In addition, one disease does not exclude another (there are cases when a tooth is surrounded by inflamed bone on all sides and it is almost impossible to say with certainty what is primary: periodontitis or periodontitis).
An x-ray is required to make a correct diagnosis and choose treatment tactics. In the image with gingivitis, we will not see any changes at all, but with periodontitis, areas where there is no bone tissue will be visible, while the teeth will be either healthy or well treated.
Treatment
It must be said right away that gingivitis is a reversible process, and periodontitis cannot be completely cured in most cases (it can be stopped, put into remission, but growing back the height of the bone is very problematic, and in many cases it is completely impossible).
If in the case of periodontitis we were dealing with microbes inside the root canal, then here we also have a microbial infection, only it is localized in the gums and bone. Treatment should be aimed at combating the cause, so the following measures can be taken:
- mandatory professional hygiene – removal of soft and hard dental plaque, polishing the surface of teeth, removal of granulations from periodontal pockets;
- correction of fillings and orthopedic structures, creation of normal contact points between teeth;
- if there is mobility of the teeth, they need to be splinted (limit movement);
- active anti-inflammatory therapy (rinses, dressings, ointments with antimicrobial action, in severe cases - antibiotics);
- general therapy (at the doctor’s discretion and depending on the severity of the process, antihistamines, painkillers, immunostimulants, vitamins, etc. can be added).
Usually this is enough to stop suppuration and relieve the acute process. To prevent exacerbations in the future, it is imperative to maintain hygiene (remove tartar at least once every six months), restore the dentition (if some teeth are missing), correct the bite (if there are problems with this) and maintain general health (if the cause of periodontitis is some common diseases).
Medical Quotes
- Guido Property (eng. Guido Majno), author of the famous book “Healing Hand; Man and Wound in the Ancient World":
“That's why pus is a noble substance: it's made of brave cells that will never go back into the blood vessels to run again, they all died in the line of duty. Let us also note the double meaning of suppuration: it means that there is an infection, but also that the body is fighting it well. The outcome of the battle can be guessed, to some extent, by the nature of the pus, as was observed even in ancient times. A whitish, creamy character (and therefore rich in polynuclear cells) is “best” because it means the infection is controlled effectively. Hence, its ancient Latin name is “pus bonum et litudabile” (good and praiseworthy pus). Liquid or smelly pus indicates poor protection or particularly virulent bacteria. »
“Pus is therefore a noble substance: it is made of brave cells that never sneak back into the blood vessels to escape; they all die in the line of duty. Note also the double meaning of suppuration: it indicates that there is an infection, but also that the body is fighting it well. The outcome of the battle can be predicted, to some extent, from the aspect of the pus, as was observed even in ancient times. The whitish, creamy kind (and therefore rich in polys) is “preferable,“ because it indicates that an infection is being fought effectively. Hence its ancient Latin name of pus bonum et litudabile. "Good and laudable pus." Thin or malodorous pus suggests a poor defense or especially vicious bacteria. »
- Sergei Yudin (Russian: Yudin Sergei), author of the book “Reflections of a Surgeon”
“... I see how the resident, like some kind of tormentor, approaches the patient with a probe and an “oncotome” in his hands; I hear these screams, tearing my soul, when, noticing the swim, he begins to examine with a probe “the direction of the stroke” and immediately makes a cut between the dirty sheets and is glad that “pus bonum et laudabile” is flowing. We finished dressing on one bed, moved to another, and here it was the same: probe, screams, pus, stench ... "
“... I see how the resident, like some kind of tormentor, approaches the patient with a probe and an “oncotome” in his hands; I hear these soul-rending screams when, noticing a leak, he begins to examine the “direction of movement” with a probe and immediately makes a cut between the dirty sheets and is glad that “pus bonum et laudabile” is flowing. They finished dressing on one bed, moved to another, and here it was the same: probe, screams, pus, stench ... "
How to treat an abscess on the gum with folk remedies?
In both cases, the cause of the development of the process is an infection that sits deep in the gum or bone. This means that we still won’t be able to influence it directly. Traditional methods (rinsing with herbs, applying propolis, etc.) usually bring their results: the fistula really goes away for a while. BUT! All these methods remove the effect, not the cause! Until the microbial contamination is removed, inflammation will progress. It won’t cause such discomfort, but it certainly won’t go away on its own.
Therefore, treatment should begin with a visit to the dentist to determine the cause. And only then, when you identify the cause and begin to fight it together with the doctor, you can also use traditional therapy, since rinsing with herbs really gives a good result after removing the stone, and, for example, sea buckthorn oil slightly speeds up the healing of wounds on the mucous membrane.