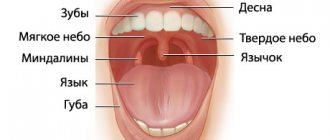
What is the tongue silent about? Yes, yes, today we will tell you about a small conical-shaped process that hangs over the root of the tongue. Why, in fact, about him? This topic was prompted by a question from one of the patients: “why is it needed, this tongue?” And we thought, why not tell us more about it. After all, practically no one pays attention to him! Nevertheless, the tongue performs many important functions! And we decided to restore justice! So, the uvula, or uvula palatine, is a small conical process of the posterior edge of the soft palate, consisting of connective tissue.
Functions of the uvula
Firstly, our tongue is able to separate air flows and sets their further direction of movement. Because it is a continuation of the soft palate. And the soft palate, when functioning normally and largely thanks to the tongue indicator, is a natural partition between the oral and nasal cavities.
Secondly, the tongue separates the flow of food, preventing it from entering the pharynx. Are you interested in knowing how this happens? Please! When food touches the tongue, it provokes a spasm in the throat, which prevents the person from choking. This little giant is able to trigger, if necessary, a gag reflex, saving us from intoxication. Remember? “Two fingers in your mouth?”
Thirdly, it protects, as best it can, from the penetration of a flow of cold air, warming it (the air) with its own vessels. Yes, the tongue has not only its own vessels, due to which it swells during the inflammatory process in the throat, but also its own muscles, covered with a mucous membrane.
Hypertrophy of pharyngeal lymphoid tissue
For hypertrophy of the palatine tonsils, physical methods, climatic and restorative treatment are used. If there is a sharp increase in the palatine tonsils and conservative therapy is unsuccessful, they are partially removed (tonsillotomy), in most cases simultaneously with the removal of the adenoids. The operation is performed on an outpatient basis under local anesthesia. After applying a tonsillotome to the part of the tonsil protruding from behind the arches, it is fixed with a fork and quickly removed. The postoperative regimen and prescriptions are the same as after adenotomy. The disadvantages of tonsillotomy include incomplete removal of the tonsil, especially when hyperplasia and inflammation of the tonsil are combined. The most common complications include bleeding, suppuration of the surgical wound, cervical lymphadenitis, and injury to the soft palate. Conservative treatment of adenoids is usually ineffective, and the physiotherapeutic procedures used in this case help to stimulate their growth. Timely removal of adenoids (adenotomy) eliminates the irritating effect of infected mucus from the nasopharynx on the tonsils, nasal breathing is restored, which often leads to shrinkage of the tonsils. Indications for adenotomy: frequent colds, severe disruption of nasal breathing, hypertrophy of the II and III degrees of adenoids (and if the ear is affected, also grade I adenoids, since it is necessary to free the mouth of the auditory tube), recurrent and chronic tracheobronchitis, pneumonia, bronchial asthma, recurrent and chronic diseases of the paranasal sinuses, hearing loss, secretory, recurrent and chronic otitis media, speech impairment, psychoneurological and reflex disorders (enuresis, epileptiform disorders). Contraindications to adenotomy: acute infectious diseases, their precursors or contact with patients with childhood infections. After a sore throat, an acute respiratory disease, surgery can be done after 1 month, after the flu - after 2 months, after a preventive vaccination - after 2-3 months, after chicken pox - after 3 months, after rubella, scarlet fever - after 4 months, after measles, whooping cough , mumps, infectious mononucleosis - after 6 months, after infectious hepatitis - after 1 year (after a blood test for bilirubin), after meningitis - after 2 years. Contraindications are also blood diseases (acute and chronic leukemia, hemorrhagic diathesis, immune hemopathy), carriage of toxigenic measles, non-bacteria diphtheria, acute diseases of the ENT organs or exacerbation of chronic diseases, acute diseases of internal organs or exacerbation of chronic diseases, decompensated conditions in diseases of the heart, kidneys , liver and lungs; dental caries, thymogaly, pharyngeal vascular abnormalities. Before the operation, children undergo examination, the minimum of which ensures the safety of the operation: general blood test, coagulation, bleeding time, tests to detect HIV, Australian antigen; Analysis of urine; dental sanitation, throat and nasal smear to identify toxigenic corynebacterium diphtheria bacilli; pediatrician's conclusion on the possibility of surgical intervention; lack of contact with infectious patients. The child is prescribed drugs that increase blood clotting. The operation is performed in a one-day hospital setting, under local anesthesia, using a ring-shaped knife - Beckmann's adenotom. Basket adenotome is also used. The adenotom is inserted into the nasopharynx strictly along the midline, then moved upward and anteriorly to the posterior edge of the nasal septum, and the upper edge of the instrument is pressed against the dome of the nasopharynx. In this case, the adenoid tissue enters the adenoid ring (Fig. 4.3, see color insert). The adenoid is quickly and sharply moved anteriorly and downward, cutting off the adenoids. In children, adenoid growths are often combined with hypertrophy of the palatine tonsils. In these cases, tonsillotomy and adenotomy are performed simultaneously. After 3 hours, if there is no bleeding after a follow-up examination, the child is discharged home with a recommendation of a home regimen, a gentle diet, and taking blood clotting agents and sulfonamide drugs. In recent years, endoscopic adenotomy under anesthesia has been introduced into practice, under conditions of suspended pharyngoscopy with visual control of an endoscope inserted into the posterior sections of the nasal cavity. With adenotomy, the following complications are possible: anaphylactic reaction to an anesthetic, bleeding. The severity of bleeding after adenotomy is assessed by the level of hemoglobin, hematocrit, blood pressure and pulse. If there is bleeding after adenotomy, a repeat adenotomy is performed to remove remnants of the adenoids, and general and local hemostatic measures are carried out. Complications also include suppuration of the surgical wound with the development of regional lymphadenitis, retropharyngeal, parapharyngeal abscess, mediastinitis, sepsis, asphyxia during aspiration of a removed adenoid, injury to the soft palate with the subsequent development of its paralysis and symptoms of dysphagia and dysphonia, injury to the root of the tongue, which is usually accompanied by severe bleeding, aspiration pneumonia.
Surgical treatment of hypertrophy of tonsils and adenoids
In the Republic of Belarus, the concept of informed voluntary consent to medical intervention is reflected in Articles 27, 28, 29 and 30 of the Law on Health Care, which lists the general rights of the patient, in particular: the right to choose a doctor, informed voluntary consent, refusal of medical intervention, the right to information about your health and all aspects of medical interventions proposed or carried out.
From the point of view of medical law, informed consent to medical intervention should be understood as the patient’s voluntary, competent acceptance of the proposed treatment option. This decision should be based on receiving complete, objective and comprehensive information about the upcoming treatment, its possible complications and alternative treatment methods.
In accordance with the above provisions, we invite you to familiarize yourself with the principles and methods of surgical treatment of hypertrophy of the tonsils and adenoids. The written information provided to you serves this purpose. Read it carefully to discuss any unclear points with your doctor.
General concepts about tonsillitis, tonsil hypertrophy and adenoids.
Every healthy child has lymphoid tissue in the pharynx, which is united into the so-called lymphadenoid pharyngeal ring. It includes the palatine tonsils - “tonsils” - they can be seen when examining the mouth - they look like balls protruding on the sides of the tongue, the pharyngeal tonsil - it cannot be seen during a direct examination of the oral cavity, it hides in the nasopharynx, behind the palate, lingual tonsil - located at the root of the tongue, and many lymphoid follicles scattered along the back wall of the pharynx, at the entrance to the larynx. These formations help the child defeat pathogenic bacteria that enter the throat during breathing and eating, and contribute to the formation of local immunity - protection against pathogens. By the way, in these organs there are no cells that affect the sexual development of the child, they do not produce sex hormones, therefore their diseases do not affect the sexual development of the child, and if they are removed if necessary (more on this later), sexual development is not disrupted.
Location of adenoid vegetations in the nasopharynx (adenoid vegetations are highlighted in red)
In early childhood - usually from 2 to 5-7 years - the described organs work very hard, as the child expands the scope of contacts with peers by attending kindergarten, and inevitably often becomes infected and develops respiratory diseases. Moreover, if the child’s immune forces are not strong enough due to congenital characteristics, environmental factors and other reasons, the lymphoid organs increase in volume. This enlargement of the palatine tonsils is called “hypertrophy of the palatine tonsils”; they can become inflamed - inflammation of the tonsils is called tonsillitis. An enlarged, chronically inflamed pharyngeal tonsil is called “adenoids.”
Adenoids have a significant impact on health and the development of nearby organs. What kind of influence is this? A chronic inflammatory process, constantly smoldering in the adenoid tissue, periodically exacerbating, contributes to protracted, recurrent diseases of the trachea and bronchi (bronchitis, obstructive bronchitis, tracheitis, pharyngitis), can independently cause or aggravate the course of allergies, in severe cases manifested in the form of bronchial asthma, allergic rhinopathy, atopic dermatitis.
Adenoids, filling the nasopharynx, cause difficulty in nasal breathing, impair the functioning of the auditory tubes, which cannot sufficiently deliver air to the middle ear, as a result of which secretory otitis media develops, which can lead to hearing loss, and if an infection enters the ear, to acute hearing loss. inflammation – acute purulent otitis media. A noticeable obstacle to the passage of an air stream through the nose leads to breathing through the mouth, and, consequently, to the fact that the nose cannot perform its functions, which, in turn, are very important. The consequence is obvious - untreated air enters the respiratory tract - not purified, not warmed and not humidified. And this greatly increases the likelihood of inflammatory processes in the pharynx, larynx, trachea, bronchi, and lungs (tonsillitis, laryngitis, tracheitis, bronchitis, pneumonia).
Poor breathing through the nose contributes to improper development of the maxillofacial area - the bite of the teeth is disrupted, the shape of the face changes (the so-called “adenoid face”), the paranasal sinuses develop poorly, which in primary school age leads to sinusitis - sinusitis (sinusitis, sinusitis). , ethmoiditis), and later – to chronic sinusitis, the growth of polyps in the sinuses and nasal cavity.
What factors contribute to the appearance of adenoids?
- Heredity - at least if the parents suffered from adenoids, the child, to one degree or another, will also encounter this problem.
- Inflammatory diseases of the nose, throat, pharynx - and respiratory viral infections, and measles, and whooping cough, and scarlet fever, and tonsillitis, etc.
- Eating disorders - especially overfeeding.
- Tendency to allergic reactions, congenital and acquired immunity deficiency.
- Violations of the optimal properties of the air that the child breathes - very warm, very dry, a lot of dust, an admixture of harmful substances (ecological conditions, excess household chemicals).
Thus, the actions of parents aimed at preventing adenoids come down to correction, and even better, to the initial organization of a lifestyle that promotes the normal functioning of the immune system - feeding according to appetite, physical activity, hardening, limiting contact with dust and household chemicals.
If the child, along with the adenoids, has enlarged tonsils
At the age of 8-9 years, when a child has enlargement (hypertrophy) of the palatine tonsils, but has not yet developed chronic tonsillitis (the child does not suffer from sore throats, purulent plugs do not accumulate in the lacunae), it is possible to reduce them using minimal surgical intervention on the tonsils volume and stop the pathological process. In this case, otolaryngologists suggest that when removing the adenoids, the palatine tonsils are also reduced in volume (“cut”) - this operation is called tonsillotomy. If this is not done, the child has a high probability of even greater enlargement of the palatine tonsils (so-called compensatory hypertrophy), which will negate the results of adenotomy - again the child will begin to breathe poorly through the nose, get sick often, snoring will not go away or will get worse. In addition, against the background of hypertrophy, a chronic inflammatory process often develops in the palatine tonsils, which subsequently requires their complete removal.
Tonsillitis can be acute or chronic. Acute tonsillitis - tonsillitis - is an infectious disease that requires conservative (drug) treatment at home or in an infectious diseases hospital under the supervision of a pediatrician. The causative agents of infectious diseases of the respiratory tract (most often streptococci) after a sore throat remain in the palatine tonsils, and their chronic inflammation develops - chronic tonsillitis. Under unfavorable circumstances (hypothermia, stress, viral infection), the process in the tonsils is activated. This occurs in the form of another sore throat with plaque on the tonsils or purulent plugs. What is very dangerous is that each exacerbation of tonsillitis can cause complications in the form of diseases of other organs and systems of the child’s body, most often rheumatic diseases of the heart and joints, kidney diseases (pyelitis, pyelonephritis, glomerulonephritis). In addition, exacerbation of tonsillitis or tonsillitis sometimes causes complications in the form of an abscess (ulcer) in the pharynx. This complication is called peritonsillar abscess.
In chronic tonsillitis, the course of the disease can go so far that the tonsils cease to perform their protective function; this form of tonsillitis is called “decompensated” and cannot be cured with medications; it requires surgical treatment - removal of the tonsils. The operation to remove the tonsils is called a tonsillectomy.
When should you consult an ENT doctor so that it is not too late?
If your child begins to get a “runny nose” frequently and it lasts longer than 10-12 days, the child, even in a state of relative health, begins to breathe worse through his nose, snores during sleep, and begins to be unable to hear (the child becomes inattentive, asks questions again, asks to increase the volume when watching TV programs ), you should visit an otolaryngologist to assess the condition of the pharynx, determine the presence of adenoids and the degree of their enlargement.
How does a doctor determine whether a child has adenoids and what size they are?
This is done using a small round mirror inserted behind the soft palate (this is difficult to do in young children), or by digital examination of the nasopharynx: the doctor feels the nasopharynx with his finger for 1-2 seconds. This is the most reliable, reliable and safe method for diagnosing adenoids. An X-ray examination is also used - a lateral radiograph of the nasopharynx using a contrast agent that is instilled into the nose, an endoscopic examination - examination of the posterior parts of the nose and nasopharynx with rigid or flexible endoscopes after anesthesia of the mucous membrane - a painful procedure for young children and therefore used in cases that are difficult to diagnose cases (for example, with congenital underdevelopment of the nasal passages, suspected tumor, etc.).
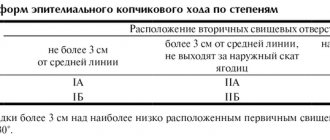
The size of the adenoids is assessed in degrees - there are three of them: the first - when the adenoids occupy a third of the volume of the nasopharynx, the second - two-thirds, and the third - when the adenoids fill the entire nasopharynx.
The grade is determined to evaluate changes in the adenoids during treatment, and not to decide whether to remove them or not. Indications for adenoid removal are determined by other criteria. More on this later.
Is it possible and necessary to “treat adenoids”?
We emphasize that it is not only possible, but also necessary to treat, but not the adenoids, but the chronic inflammatory process in them, called adenoiditis. Until the child develops the changes mentioned earlier, both local treatment should be used in the form of drops, irrigation of the nasal mucosa and nasopharynx with aqueous solutions that have anti-inflammatory, antiallergic and antimicrobial properties, as well as general treatment methods, including vitamin preparations, agents, those affecting the immune system, locally acting vaccine preparations, physiotherapeutic methods (magnetic and laser therapy, inhalation methods of drug administration have proven themselves well). Homeopathic methods of treatment are not contraindicated. However, when, during observation of a child, changes appear in the ears (recurrent otitis, dysfunction of the auditory tubes, exudative otitis), paranasal sinuses (recurrent sinusitis, chronic sinusitis), there are chronic or recurrent bronchopulmonary diseases, allergies, adenoids, regardless of the degree of their increase are subject to mandatory removal.
How urgently should the operation be performed?
Operations to remove adenoids and tonsils - adenotomy, tonsillotomy, tonsillectomy - are planned, that is, they are performed when the child is in full health or in remission of chronic diseases. It cannot be performed during acute illnesses (ARI) and 3-4 weeks after recovery. Thus, it is always possible to perform this operation in a period favorable for the child, which will minimize the risk of postoperative complications.
Is it possible to delay or not do the operation at all, because, they say, the adenoids are resolving, maybe they will “outgrow”?
Indeed, adenoid tissue atrophies over time, however, this process begins in adolescence and ends at 18-20 years of age. This process is long, and by the time it is completed, as a rule, a number of irreversible diseases requiring surgical treatment have formed (chronic otitis media, sinusitis, tonsillitis). Thus, it is obvious that it is more expedient to perform a minor operation in early childhood and improve the child’s health than to condemn him to long-term treatment, which often does not lead to full health, at an older age.
Do adenoids grow back, are relapses common?
Yes, adenoids can recur.
We draw attention to the fact that, regardless of the qualifications of the surgeon, it is impossible to completely remove the pharyngeal tonsil - at least something will remain. And there is always a possibility that adenoids will appear (grow) again. This happens quite rarely - in 4-5% of cases. However, relapse does not mean repeated surgical treatment. As a rule, adenoid tissue can reappear in the nasopharynx no earlier than after 7-12 months, during which time the function of the auditory tubes and nose usually has time to recover, the volume of the nasopharynx increases as the child grows, and the newly enlarged adenoids no longer have such a detrimental effect, as before the operation. Typically, conservative treatment methods can solve the problem. Repeated adenoid removal is required in 1-2 patients out of a thousand operated on.
The reappearance of adenoids is a reason for serious parental consideration. And it’s not at all about the fact that a bad doctor was “caught”. And the fact that all doctors taken together will not help if the child is surrounded by dust, dry and warm air, if the child is fed with persuasion, if TV is more important than walks, if there is no physical activity, if... If it is easier for mom and dad to take the child to otolaryngologist, than to part with your favorite carpet, organize hardening, sports, sufficient time in the fresh air.
Removed tonsils cannot grow back. Tonsillectomy allows you to radically and permanently solve the tonsillar problem.
How are adenoids removed?
This operation is performed in children under 8 years of age without local anesthesia; for children over 8 years of age, anesthesia is used by lubricating or irrigating the nasopharyngeal mucosa with a lidocaine solution. In young children this is prohibited due to the possibility of asphyxia (suffocation) developing in the child. This operation is unpleasant, but not painful; the sensations experienced by the child are comparable to lubricating the throat. It lasts a short time (5-6 seconds) and, with proper psychological preparation of the child, is tolerated satisfactorily. Under special circumstances - the presence of concomitant diseases in which local anesthesia is undesirable, the child’s pronounced negativism towards medical manipulations, emotional lability and psychological unpreparedness of the child and parents for surgery without anesthesia - adenotomy and tonsillotomy are performed under general anesthesia, which involves a more in-depth examination of the child.
The simplicity of the operation does not indicate the safety of the operation. Complications due to anesthesia, bleeding, and damage to the palate are also possible. But all this does not happen often. You can find a list of possible complications below.
Surgeons have long abandoned the removal of adenoids using ultrasound and laser due to the huge risk of complications.
How long does a child stay in the hospital after adenotomy and tonsillotomy?
Due to the high risk of bleeding in the postoperative period, we recommend staying in the hospital for 24 hours after surgery to remove adenoids. Usually the child is discharged home the next day. After tonsillotomy, the child is observed in the hospital for a day longer.
What should you do after your baby is discharged?
The child is discharged from the hospital under the supervision of an ENT doctor or pediatrician at the clinic at the place of residence. Home treatment is usually recommended for 3-5 days.
In this case, physical activity should be limited, however, there is no need to keep the child in bed. When eating during the first days, you should not eat hot, spicy foods, sour juices and fruits, carbonated drinks, or ice cream. After 3-5 days, the diet becomes normal. 3-5 days after discharge, if the child’s general condition is satisfactory, there is no elevated body temperature, and the wound in the pharynx is healing smoothly, you can visit the children’s group and go outside. You can’t just do sports or go to the pool. The wound in the nasopharynx heals completely in 2-3 weeks. A month after the operation, there are no restrictions in lifestyle or diet.
How to remove adenoids at the Children's City ENT Center?
To establish a diagnosis, if there is no ENT doctor in the clinic, you can make an appointment at the city ENT consultation office by calling 2-78-49-00 (inquiry). Consultative reception is carried out on weekdays, from 8.00. until 20.00.
If the diagnosis of “hypertrophy of the palatine tonsils, adenoids” has been established and the decision to operate on the child has been made, with a referral for surgical treatment issued at the clinic, you should go to the emergency department of the 3rd Children's Clinical Hospital at any time convenient for you. Your child will be registered for hospitalization on the day you choose and will be given an examination plan (a list of tests necessary to perform the operation). Hospitalization is carried out on Tuesday and Thursday, from 13.00. until 15.00. and on Sunday from 16.00. until 18.00. During hospitalization, the child is examined by an ENT doctor, who evaluates the examination performed in the clinic in accordance with the scope of surgical treatment and the method of anesthesia and, in the absence of contraindications to the operation, admits the child to the hospital. The operation is carried out the next day. Mothers with children under 5 years of age are hospitalized and issued a certificate of incapacity for work.
Clinical picture
Hypertrophied palatine tonsils have a pale pink color, a smooth surface, clearly defined lacunae and a loose consistency.
They protrude somewhat beyond the edges of the anterior palatine arches. Patients complain of coughing, difficulty swallowing and breathing. There may be a speech disorder that occurs due to changes in the upper resonator, as a result of which the voice becomes nasal. Make an appointment right now!
Call us by phone or use the feedback form
Sign up
Due to brain hypoxia (oxygen starvation), patients sleep very restlessly at night, insomnia and night cough are possible. As a result of relaxation of the pharyngeal muscles, attacks of obstructive apnea (temporary cessation of breathing during sleep) may occur. Due to tubular dysfunction (the initial stage of dysfunction of the system), hearing impairment occurs, and the formation of exudative otitis media (ear inflammation) is possible.
Treatment
If there are complaints of difficulty swallowing and breathing, cough, or speech disorders, it is recommended to partially remove the tonsils (tonsillotomy) when the child reaches 5-7 years of age.
But such an operation has the following contraindications: acute infectious diseases, blood diseases, diphtheria bacilli carriage. Tonsillotomy is not recommended for polio outbreaks. ENT surgery can be performed on an outpatient or inpatient basis, both under anesthesia and local anesthesia. It is not uncommon to perform a bilateral tonsillectomy - complete removal of the tonsils.