Are “bad teeth” a hereditary factor?
The concept of “bad teeth” implies:
- thinned enamel;
- congenital abrasion of teeth;
- malocclusion and its pathologies;
- hypersthesia - a reaction to high and low temperatures;
- formation of tartar and plaque deposition;
- yellow or brownish discoloration of teeth from birth.
What genes influence:
- tooth structure;
- shape;
- enamel color;
- bite structure;
- metabolism in the body.
A set of human genes is also responsible for the health and beauty of teeth. A set of human genes is also responsible for the health and beauty of teeth. The combination of these factors influences the predisposition to the development of caries. For example, if the fissures (grooves on the surface) of the chewing tooth are deep, food debris is difficult to remove, pathogenic microflora develops, which quickly leads to fissure caries.
The child will inherit genes from his parents. And along with them, all the genetic information of previous generations. Therefore, unfortunately, healthy teeth from parents directly do not guarantee the same good teeth in children, since they may inherit the genome of their grandmother or grandfather. In addition, the genes themselves manifest themselves differently depending on external factors and combinations of parental genotypes for recessive and dominant genes.
Under the influence of long-term living in unfavorable environmental conditions, increased background radiation and unbalanced nutrition, genetic changes occur that affect the dental health of descendants.
What is transmitted genetically
Most diseases of the dental system are not 100% genetically dependent. However, there are signs that are passed on from generation to generation and can ultimately affect the condition of the teeth. These include:
- composition, thickness and shade of enamel;
- shape of dental units;
- bite geometry;
- timing of the eruption of primary and permanent teeth;
- composition of saliva and oral microflora.
Along with these characteristics, the child also inherits a predisposition to certain pathologies. But there is no fatality in this. With a reasonable, competent attitude to oral care, you can avoid the development of one or another disease, the likelihood of which is genetically predetermined.
Other factors affecting dental health
Heredity is just one factor. The influence on the human body in general and teeth in particular is exerted by:
- ecological situation;
- food intake and diet;
- Lifestyle;
- regular anxiety and repetitive stress;
- smoking, drinking alcohol, other bad habits;
- woman's behavior during pregnancy;
- infant habits of sucking fingers, pacifiers and other objects.
Even if there are relatives with an “ideal” tooth structure and an even bite, the lifestyle of the expectant mother will affect the formation of tooth buds in the fetus.
During pregnancy, people think about the health of the baby’s body and teeth. That's why:
- treat emerging diseases in a timely manner;
- regularly observe the rules of oral hygiene;
- do not use medications without the consent of your doctor - some of them can affect the color and thickness of enamel, for example, tetracycline;
- balance your diet, eat healthy foods and avoid unhealthy ones;
- normalize your sleep schedule, do not overexert yourself physically.
Anomalies of dental development - symptoms and treatment
Treatment depends on the type of anomaly and may include tooth extraction, prosthetics with crowns and veneers, surgical and therapeutic intervention.
Supernumerary teeth must be removed. If the crown or root part of adjacent teeth is abnormal or destroyed due to a pathological process, then after a thorough examination the corresponding complete tooth is removed, and the supernumerary one is moved into the dentition. Supernumerary teeth most often have irregular shape, size or structure, so treatment is often completed with restoration with composite material or the creation of an artificial crown or veneer.
for patients with hypodentia and edentia . Partial absence of teeth, as a rule, is combined with a violation of the position of adjacent teeth and antagonist teeth, as well as with anomalies in the shape and size of the dental arches. Therapy will consist of orthodontic correction followed by prosthetics and implantation [7]. Patients with true primary edentia are very rare; they should wear complete removable dentures from an early age. Children often respond well to prosthetics and quickly adapt to them. Due to dynamic age-related changes occurring in the dental system, all removable dentures are replaced with new ones every 1.5-2 years. When making dentures, the doctor and technician take into account the morphological and functional characteristics of the dental system.
Treatment of anomalies in tooth size (macro- and microdentia) is usually orthopedic. If macrodentia and microdentia are combined with anomalies in the shape and size of the dentition, malocclusion, then preliminary orthodontic preparation will be required. It consists in the correct placement of teeth and allows you to subsequently qualitatively restore the desired tooth anatomy with crowns or veneers. In case of mild pathology with a small difference in the height or width of the teeth and their normal relationship with the size of the jaws and the type of face, orthodontic treatment can be limited.
Treatment of patients with abnormal tooth shapes involves performing composite restorations and making crowns or veneers that restore the anatomical shape. For concomitant pathologies that require correction of the bite, shape and size of the dental arches, orthodontic preparation will be required.
Treatment of anomalies in the structure of hard dental tissues (hypoplasia, hyperplasia, hypercementosis, amelogenesis imperfecta, medicinal and toxic effects on dental tissues, etc.) is complex and includes therapeutic, orthopedic and orthodontic care.
Treatment of teething anomalies . Early eruption of primary teeth usually does not require orthodontic intervention. If there is a violation, it may be necessary to switch to artificial nutrition instead of breastfeeding. Early eruption of permanent teeth is often caused by untimely loss of baby teeth. It often requires correction of the position of adjacent teeth and antagonist teeth to prevent complications. If the permanent tooth has already erupted, but the baby tooth has not yet fallen out, then the latter is removed, and the direction of eruption of the permanent tooth is corrected, if necessary.
For late eruption of primary teeth, gum massage will be helpful. Delayed eruption of a permanent tooth is usually corrected by an orthodontist. To do this, orthodontic preparation is carried out on the brace system: a place is created for the impacted tooth and a support is prepared for its traction. If it is necessary to open or remove an impacted tooth, the treatment is carried out by a surgeon [1].
Anomalies in the position of teeth are corrected using prosthetics with veneers and crowns, therapeutic restoration and orthodontic treatment with removable (in childhood) and non-removable devices: aligners and brace systems.
Necessary prevention
Beyond heredity, preventative measures to maintain dental health are everyone’s first priority. No matter how smooth and snow-white the teeth are, insufficient hygienic care leads to tooth loss.
When teeth are forming in the womb, the following are likely to occur:
- hypoplasia (underdevelopment) of enamel;
- hyperplasia (excessive formation) of enamel;
- fluorosis (intoxication with fluoride salts);
- drug-induced tissue development disorders;
- hereditary disorders.
These pathologies are predetermined, because the lifestyle of a pregnant woman leads to their appearance. In all other cases, preventive measures and hygiene will keep teeth healthy, even with bad hereditary factors.
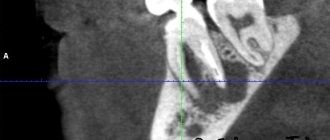
Disorders of enamel maturation with hypoplasia and taurodontism
Some experts combine it with hypomaturation, others separate it separately. The formation of enamel tissue is disrupted during tissue differentiation. The pathology may be accompanied by grooved or thin hypoplasia.
The enamel turns into various colors - from white and yellow to unpleasant brown, becomes covered with opaque specks and acquires a pathological tendency to abrasion. The photographs show large cavities in the incisors and symptoms of taurodontism. In multi-rooted teeth, the pulp cavity is expanded and the crown is lengthened. The root is short, and the distance from the occlusal surface to the bifurcation zone is increased.
Classification of dental hypoplasia
There are, especially in foreign practice, many types of classifications of this pathology, and in particular, classifications of dental enamel hypoplasia . The most generally accepted classification in the form of summarized data is presented in the table below.
| Classifying features | Type or type of non-carious lesion |
| The presence or absence of an inherited defect of a gene or genes (gene breakdown) | Hereditary hypoplasia . As a rule, all teeth are affected. Acquired hypoplasia . Due to exposure to external factors in the prenatal (before birth) or postnatal (after birth) period. The degree of damage is proportional to the duration of exposure to such factors and the severity of the underlying disease. |
| Prevalence of hypoplastic lesion | Systemic hypoplasia. Almost all teeth are involved. Localized. Focal – group lesion, local – one or two teeth. Aplasia . Certain areas are completely devoid of enamel. |
| Specific hard tissue involvement | The entire tooth is affected (especially in systemic cases). Mostly enamel, or dentin, or cement are affected |
| Clinical picture (or forms) | Spotted. There are stains on the enamel. Erosive. Cup-shaped recesses of various external shapes and depths. Sulcata . Linear grooves horizontal to the upper edge of the teeth. |
| Development period | Damage to primary or permanent teeth |
Among all forms of this pathology, the greatest and most overwhelming prevalence is tooth enamel hypoplasia . According to statistics, hypoplasia of the enamel of permanent teeth in a spotted form in varying degrees of damage affects up to 5-15% of children. The prevalence of symptoms of hypoplastic enamel defects among adolescents and young people, according to some data, reaches 47-50%.
Diagnosis of fluorosis
A dentist can distinguish fluorosis at the initial stage from caries:
- Caries manifests itself asymmetrically, while fluorosis occurs on symmetrical teeth.
- Caries has typical places of manifestation: contact surfaces of teeth, cervical areas. Fluorosis, on the contrary, appears more often on the outer surface of the teeth.
- Caries, like fluorosis, can be multiple, but still, as a rule, with caries you can see only a few affected teeth, and with fluorosis there are more of them.
- The dentist will identify fluorosis by the characteristic shape of the lesions (striations, spots).
- Caries appears on the teeth gradually, but fluorosis is visible already at the moment of teething.
Meet our tooth fairies and check prices.