Causes
The reasons for the formation of a through communication between the oral cavity and the nasopharynx are various. This is a tooth extraction carried out with disturbances or complications, pathological processes. Perforation when removing the first or second molar or premolar occurs for the following reasons:
- improperly formed socket;
- violations during tooth extraction;
- anatomical features of the upper jaw, low location of the sinus floor;
- pathological processes causing destruction of tissue, bone septum;
- cysts, tumor processes, chronic periodontitis.
Symptoms of pathology
Clinical picture of the presence of an oroantral defect:
- The appearance of bloody foam in the cavity of the extracted tooth;
- Bleeding from the paranasal sinus;
- Changing the timbre of the voice (pronunciation);
- Entry of fluid from the oral cavity into the nasal cavity;
- Changes in olfactory sensations.
The consequence of an open message that was not subject to timely diagnosis and treatment can be chronic sinusitis.
The choice of method for plastic closure of the oroantral anastomosis depends on its location, size, presence or absence of teeth on the damaged surface of the alveolar process.
There are 4 types of oroantral communication:
- Palatine
- Palatovestibular;
- Vestibular
- Located at the top of the alveolar ridge.
The diagnosis is made based on the listed symptoms and a positive laboratory test.
Diagnostics
To identify pathology, the doctor prescribes diagnostics - a nasal test and x-ray examination. The test is carried out quite simply: the patient pinches his nose, after which he is asked to take a deep nasal exhalation. If there is a perforation, a stream of air enters the mouth, and a foamy, bloody liquid appears on the hole. With the help of X-rays, the doctor has the opportunity to examine the pathology inside, determine the location and extent of the lesion, and see all extraneous fragments.
Types of operations
Methods of operations for various localizations of the defect:
- Vestibular anastomosis and anastomosis localized at the apex of the alveolar ridge.
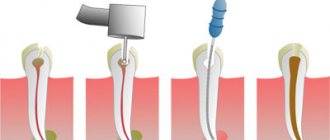
Plastic closure of the oroantral communication is performed with a trapezoidal mucoperiosteal flap cut from the surface of the alveolar process and the transitional fold of the vault of the oral vestibule in the area where the anastomosis is located.
The choice of method is due to the ease of implementation, the use of tissues of the same type, and the absence of damage to the periosteum, which has a beneficial effect on the speed of healing and replacement of the anastomosis with secondary bone.
- Palatal and palato-vestibular communications.
Most often they have relatively large (up to 10 mm) sizes. To close perforations of this type of communication, a method is used using an L-shaped palatal mucoperiosteal flap, which, when installed on the damaged surface, is fixed with sutures made of silk threads. The described method is also universal - it is suitable for damage of any severity and is easy to implement.
Treatment methods
Treatment of pathology is carried out using various methods:
- moving the flap from the mucous periosteal region of the cheek;
- covering with membranes;
- plastic surgery of the anterior wall for sinusitis.
The choice of method depends on the characteristics and course of the disease. The doctor conducts a preliminary examination and determines what the treatment will be. The main goal is to eliminate the message, reduce injuries and eliminate the development of relapses. The method is effective and shows good results. The downside is additional tissue trauma when harvesting a flap with subsequent suturing.
Repositioning the flap from the periosteal region is a popular method that is highly effective. The doctor first determines the place where the donor flap will be taken, collects it and sutures the wound. Next, the flap is transferred to the surgical area, and new tissue is formed. The treatment is carried out in two stages; in the communication area, the trapezoidal flap is attached with sutures.
The membrane is used under local anesthesia. For work, a flap of the periosteal part is cut out, which is then shifted upward. Next, the frontal part is opened slightly, the doctor performs trepanation, maxillary sinusotomy and removes all foreign tissue. The area is tamponed, the doctor installs a turunda, leaving the end protruding from the nasal passage. To maintain mobility, the flap at the base is trimmed slightly, and the opening is closed with a membrane. The defect is overlapped by 3 millimeters, then the pathological area is closed, and interrupted sutures are applied. The membrane dissolves as it heals, which is an advantage of this method.
Plastic surgery for frontal sinusitis involves submucosal resection of the nasal septum with luxation of the median concha and a retrograde incision for the lower element of the branch. This opens access to the anastomosis and provides ease of work. It is this area that is usually affected by polyps, so in parallel with the main treatment, the doctor removes foreign inclusions with thickened mucous tissue.
The next step is an arched cavity incision from the middle of the eyebrow to the transition to the slope of the nose, dissection of the periosteum with exposure of the sinus. The doctor performs an inspection of the sinus with a chisel, removing the affected mucous membrane, polyps, granulants, and accumulations of pus. During work, it is necessary to preserve as much healthy tissue as possible, which requires a certain amount of experience from the doctor.
At the final stage, the patency of the nasal canal is checked under the control of an endoscope. If there are no complications, the tissues are sutured, a cosmetic suture is placed on the face, which allows maintaining external aesthetics.
Using a flap
The treatment technique using a trapezoidal mucoperiosteal flap includes the following steps:
- determining the area where the flap will be taken, cutting it out;
- excision of the walls of the fistula and installation of the flap in place;
- covering the anastomosis, suturing the edges.
The technique is specially developed for the treatment of such pathology. It places special demands on the doctor’s hoof and strict adherence to the surgical protocol.
The doctor cuts out a trapezoidal flap; the donor site is the mucous tissue of the periosteal region. If there are indications, a maxillary sinusotomy is performed, that is, all tissues with signs of pathological damage and foreign inclusions are removed from the sinus cavity. The edges are refreshed, and curettage is performed before treating the hole with antiseptics. The differences between the method are:
- formation of lining in the sinus cavity, subsequent lining of the membrane at the mouth;
- formation of a layer by displacing the flap to the defect area;
- suturing according to the U-shaped principle, which ensures accelerated healing of the surgical area.
Result:
- layers of tissue are formed with a significant increase in quality;
- the development of relapses is prevented;
- eliminates the need for repeated intervention.
The treatment method is indicated for the formation of tissue perforation during sinusitis, during general therapy for message formation.
Preventive measures
Prevention eliminates the development of the problem, but for this the patient must regularly visit the doctor and carry out sanitary measures. This allows you to prevent the development of periodontitis and maintain the integrity and structure of bone tissue. Preventive measures also include proper treatment and no scraping of the socket during tooth extraction. The doctor needs to correctly connect the edges of the gums, which allows for the formation of a blood clot inside and the formation of a protective barrier to infection.
GBOU "NIKIO im. L.I. Sverzhevsky" of the Moscow Department of Health
Oroantral fistula
The maxillary sinus is the largest of all the paranasal sinuses and is shaped like a four-sided pyramid. The lower wall of the maxillary sinus is formed by the alveolar process along the length from the first premolar to the tubercle of the upper jaw. An anatomical feature of the lower wall of the sinus is that in some cases the bone bridge between the apexes of the roots of the teeth adjacent to it and the lumen of the sinus itself can be up to 1 mm thick, and in some cases its role is played by the mucous membrane of the sinus. In our opinion, it would be advisable to distinguish between two concepts - “oroantral communication” and “oroantral fistula”. The oroantral communication is formed immediately after the violation of the seal of the maxillary sinus and in some cases, with the correct treatment tactics, does not lead to the development of traumatic sinusitis and oroantral fistula. We can talk about the presence of an oroantral fistula when the bone walls of the alveolus of the extracted tooth are epithelialized, but the seal of the sinus is not restored.
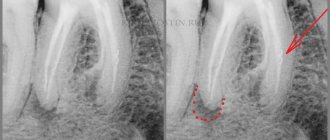
The diagnosis of chronic odontogenic maxillary sinusitis is established on the basis of clinical and radiological data. X-ray and CT examinations are the most important diagnostic methods for identifying various forms of chronic sinusitis.
The treatment tactics for chronic odontogenic maxillary sinusitis is determined by the clinical form of the disease. During exacerbation of chronic sinusitis, its exudative forms (catarrhal, serous, purulent) are treated, as a rule, conservatively. In this case, the same means and treatment methods are used that are used in the treatment of acute sinusitis. Productive forms of chronic odontogenic maxillary sinusitis (polypous, polypous-purulent) are treated surgically. Regardless of the form of chronic sinusitis in the presence of visual and intracranial complications, the main method should be surgical treatment.
The main goal of surgical treatment for chronic odontogenic maxillary sinusitis is to remove the affected teeth and create conditions for restoring the normal function of the affected maxillary sinus. To do this, regardless of the surgical approach, the damaged sinus anastomosis with the nasal cavity is created anew or restored, ensuring its free drainage and ventilation. Thus, we are talking about restoring the impaired function of the osteo-meat complex.
Treatment
There are a significant number of different options and modifications of surgical interventions on the maxillary sinuses, proposed for the treatment of sinusitis. All of them, depending on the approach, are divided into extranasal and endonasal. It should be noted that most surgeons in the surgical treatment of odontogenic maxillary sinusitis, especially in the presence of persistent oroantral communication, operate using the traditional technique of radical maxillotomy and communication plastics. Today, the technique of extra- or intranasal sinusotomy with plastic surgery of the bottom of the maxillary sinus with a trapezoidal mucoperiosteal flap cut from the vestibular surface of the alveolar process of the upper jaw is used. In some cases, sinusotomy was accompanied by the removal of a foreign body from the lumen of the sinus (most often a tooth root) or filling material.
Currently, surgical treatment of chronic odontogenic maxillary sinusitis with persistent oroantral communication in specialized clinics is carried out using a gentle endoscopic maxillotomy technique with simultaneous plastic surgery of the oroantral communication.
Endonasal operations of the paranasal sinuses were developed almost simultaneously with extranasal ones. However, only with the advent of modern endoscopes with fiber optics and long-focus operating microscopes, endonasal operations began to be introduced into clinical practice.
We fulfill
Extra- and intranasal maxillotomy with simultaneous plastic surgery of the oroantral fistula, if present.
Development factors
A through channel between the maxillary space and the mouth appears due to accidental perforation of the sinus wall. A provoking factor may be non-compliance with the technology for removing the upper premolar, first or second molar.
Provoking factors:
- Anatomical features of the structure of the upper jaw, when the bottom of the sinus is located at a low level.
- A history of a pathological process that led to the destruction of the elements of the bone wall between the root of the unit and the maxillary cavity (periodontitis, cyst, neoplasm).
- Inspection of the hole.
- Errors during intervention to remove a unit.
Diagnostic measures
Defect identification is facilitated by diagnostic procedures:
- X-ray studies.
- Nasal test.
The test allows you to reliably determine the causes of perforation. The doctor tightly pinches the patient's nose and asks him to exhale deeply through his nose. If there is an oroantral communication, a foamy liquid begins to secrete in the hole formed at the site of tooth extraction.
An x-ray allows you to see the pathology from the inside, determine its size and location.
Treatment methods
The pathology is eliminated through surgery. The choice of the appropriate method is determined by the attending physician based on the clinical picture.
- Relocation of the mucoperiosteal flap from the cheek
The technique allows you to close the perforation site and restore the aesthetics of your smile. Carrying out the manipulation requires the experience and qualifications of a doctor, accuracy and strict adherence to the protocol.
The surgeon cuts out a trapezoidal periosteal flap from the tissues of the mucous membrane. If indicated, a maxillary sinusotomy is performed. Pathologically altered tissues are removed from the inside of the sinuses. The edges of the perforation site are refreshed, curettage and disinfection of the hole are carried out.
A two-layer message delimitation is carried out:
- A lining is formed from the inside of the sinus by placing a membrane at the mouth.
- The flap is partially displaced into the defect area.
The tissues are sutured in a U-shaped manner for accelerated healing.
The technique reduces the risk of potential complications and relapse.
- Application of membranes
Under local anesthesia, the periosteal fragment is cut out and shifted upward. The frontal wall of the cavity is opened, and trepanation of the sinus is performed. A maxillary sinusotomy and amputation of foreign elements are performed.
The working area is tamponed. The turunda is installed so that the end protrudes from the nasal entrance.
To ensure mobility, the surface of the flap is incised at the base. Antiseptic treatment is carried out. The mouth is closed with a membrane.
The tissues are sutured with an interrupted suture. The membrane has the ability to self-resolve.
- Plastic surgery of the anterior wall of the frontal sinus
After anesthesia of the cavity, submucosal resection of the nasal septum is performed. Under the control of an endoscope, the doctor opens access to the frontonasal anastomosis. Polyps and thickened layers of the mucous membrane are carefully removed.
The frontal sinus is exposed. It is being reviewed. The doctor removes the affected mucous membrane, foreign objects and pus without affecting healthy tissue.
The patency of the nasal canal is checked. The tissues of the periosteum and mucosa are sutured. A cosmetic suture is applied to the surface of the face.