Periodontist
Fisenko
Marina Nikolaevna
47 years of experience
Dental surgeon of the highest category. Member of the International Federation of Dental Anesthesiology Societies IFDAS
Make an appointment
The complex of tissues surrounding the tooth and holding it in the alveolus is called periodontium. Accordingly, inflammation of these tissues in medicine is periodontitis. As this dental disease progresses, it destroys the ligaments of the tooth and the bone tissue of the jaw. Subsequently, the teeth begin to loosen and fall out, which can lead to abscesses and fistulas.
Causes
More often, periodontitis is diagnosed in middle age - 30-40 years, but today the disease is increasingly appearing in younger people, including those who have irregularly shaped teeth or bite. Pathology develops for several reasons. The main one is considered to be infection of the gums through:
- dental tissues - as a result of caries or dental plaque, which leads to the formation of tartar;
- dental pockets - against the background of gingivitis (inflammation of the gums).
Gingivitis is considered an early stage of periodontitis, since inflammation gradually spreads from the dental pockets to other tissues. The source of infection may not be in the oral cavity. Sometimes periodontitis develops against the background of other internal inflammatory diseases. The following factors can contribute to the development of periodontitis:
- smoking;
- chewing tobacco;
- hereditary predisposition;
- long-term use of antidepressants, anti-inflammatory drugs;
- treatment with immunosuppressants or calcium channel blockers (cause gingival hyperplasia);
- injury to the gums due to physical impact
- unprofessional dental treatment;
- improper prosthetics;
- insufficient oral hygiene;
- diabetes;
- changes in hormonal levels during menopause, pregnancy, lactation;
- vitamin B or C deficiency.
The development of periodontitis is also promoted by constant eating too soft food. It impairs the process of self-cleaning of teeth. Another cause of periodontitis may be the habit of chewing on only one side, since this disrupts the uniform distribution of load on the teeth.
Acute periodontitis
This phase of the disease develops either with an exacerbation of chronic periodontitis, or when infection penetrates into the periodontal pockets as a result of trauma. Teeth and gums are injured as a result of blows and bruises due to unprofessional dental intervention. Bruxism, a disease in which involuntary grinding of teeth against each other, deserves special attention when considering traumatic factors. Scientists from Okayama University conducted a study according to which most of the observed patients had varying degrees of severity of periodontitis.
There are two main subtypes of acute periodontitis: non-purulent and purulent forms. In the first case, extensive periodontal damage occurs, characterized by severe swelling of the gums, pronounced pain, a significant increase in the spaces between the teeth and gums, progressive destruction of connective tissue, exposed teeth and bleeding. The purulent form is characterized by the formation of fistulas and boils, from which, when pressed, a viscous grayish-white liquid is released, which has a characteristic unpleasant odor. It is localized in a specific area of the oral cavity, without affecting the entire gum.
Acute periodontitis is especially dangerous during pregnancy. Hormonal changes in a woman’s body provoke complications of the disease. If pus and bacteria enter the circulatory system, they can cause fetal toxicity. This can lead to congenital diseases or miscarriage in the child.
Acute periodontitis, like chronic periodontitis, can develop against the background of damage to the body by viruses. Occurring suddenly, it deprives a person of the ability to effectively brush his teeth. If you do not contact a dental clinic as soon as possible, there is a risk of a significant increase in body temperature and poisoning of the body with toxins.
Often the acute form of periodontitis requires surgical intervention. This may include removing a section of gum using a laser or scalpel under local anesthesia (gingivectomy), dissecting the gum and cleaning out the root of the tooth, opening boils and removing pus using a drainage tube.
Symptoms and signs
Periodontal inflammation is rarely accompanied by pain. More often the disease manifests itself in the form of swelling and redness of the gums. They may experience bleeding, and sometimes a local increase in temperature is observed. At an early stage, it is difficult to recognize the disease. Most patients go to the doctor with complaints of bleeding gums while brushing their teeth or eating.
If the disease is not treated, the gums subsequently begin to separate from the teeth, causing them to become longer. Significant gaps appear between the teeth. They fall out at a later stage of the disease. Other characteristic symptoms of periodontitis:
- bad breath;
- purulent discharge on the gums;
- chronic toothache;
- plaque on teeth;
- viscous saliva;
- increased gum sensitivity;
- yellow plaque on the root part of the enamel;
- sensation of pulsation in the gums.
These symptoms also affect the general condition of a person. Sometimes general weakness and headache appear, and the temperature rises.
Treatment of localized periodontitis
First, the patient's dental plaque is removed to eliminate pathogenic bacteria in the oral cavity. The main therapy is focused on the healing of periodontal tissue, gums and treatment of the cause of the disease: vitamins, antiseptics, anti-inflammatory drugs and agents to enhance immunity are prescribed. The patient is referred for examination to an immunologist, endocrinologist and gastroenterologist to prescribe concomitant therapy.
In mild and moderate stages of pathology, curettage is performed - treating gum pockets with antiseptic agents and removing deposits. The teeth are ground and tightened with a special dental splint - the loosening is stopped, and after treatment of the periodontal tissue, the teeth are again securely held in the gums.
Surgical intervention is required only in severe cases of the disease, when the depth of the periodontal pockets is more than 5 mm: excess tissue is excised and sutured. Severe mobility of teeth with exposed roots cannot be treated, and teeth must be removed.
Traditional methods without general drug therapy and dental supervision are taboo. They can alleviate the patient’s condition, but when treating even a mild stage of periodontitis only with traditional methods, the disease will very soon develop into a severe form.
However, as an addition to dental treatment you can use:
- decoctions of oak bark and nettle - for bleeding gums;
- fir and sea buckthorn oil - for severe burning and swelling of the gum tissue;
- a decoction of mint, calendula, violet - for bad breath.
Stages
During the course of the disease, there are three main stages, which differ in the nature and severity of symptoms. These are the next stages.
- First. Periodontal pockets are still shallow - up to 3 mm. Periodically, after brushing, bleeding gums are noted. It is not accompanied by pain or loosening of teeth.
- Second. The depth of the pockets increases to 5 mm, due to which the neck of the tooth is partially exposed. Hypersensitivity also occurs when eating hot or cold foods.
- Third. This stage, with a non-aggressive course of the disease, develops approximately 4-5 years after the onset of inflammation. In severe cases, the dental pockets deepen up to 6 mm. Food debris accumulates in them, which leads to suppuration. This causes the teeth to become very loose.
Types of Localized Periodontitis
By severity:
- localized periodontitis of mild severity is characterized by pain in some teeth when pressing on the gums, sometimes bleeding and the appearance of periodontal pockets, but the patient’s general well-being does not change;
- localized periodontitis of moderate severity is determined by deepening of the gum pockets, poor tooth mobility, and regular bleeding of the gums;
- localized periodontitis in a severe stage leads to complete loosening of the teeth, exposure of the roots and suppuration of the gums; the bone is so destroyed that implantation without prior extension is no longer possible.
According to the nature of the pathology:
- acute localized periodontitis develops quickly and rapidly, with the manifestation of all the characteristic symptoms - the disease is successfully treated, but without dental care it becomes chronic;
- localized chronic periodontitis is characterized by moments of exacerbation and calm; it seems to the patient that the pathology has receded, but the inflammatory process continues to destroy tissue and manifests itself in a severe stage.
Degree of tooth mobility
With periodontitis, teeth gradually become loose. Depending on their mobility, there are 4 degrees of the disease:
- 1st degree, when the tooth moves no more than 1 mm to the adjacent tooth, in the bucco-lingual and vestibulo-oral directions;
- 2 degree, in which mobility is observed in the same directions as in the first degree, but only by more than 1 mm;
- 3rd degree. Teeth become mobile in any direction, including vertical;
- 4th degree. Mobility is observed in all directions, and the tooth can even rotate around its axis.
What is localized periodontitis?
Localized, or focal, periodontitis is an inflammation of the periodontal tissues surrounding the tooth. Unlike generalized periodontitis, localized periodontitis spreads locally - it affects only one or several adjacent teeth. And even with prolonged development, the disease does not affect the “neighbors”. The disease affects all age groups, regardless of gender, but people aged 30 to 50 years and adolescents are more likely to suffer.
Diagnostics
The first stage of diagnosis is an external examination of the oral cavity. The specialist performs probing (periodontal test) - a procedure that will determine the depth of the formed dental pocket. This is necessary to establish the severity of periodontitis. Additionally, the following studies are prescribed:
- benzidine test. Allows you to identify pus in periodontal pockets without performing a microscopic examination. To do this, turunda soaked in a solution consisting of benzidine, acetic acid and polyethylene glycol is inserted into the pocket. If there is no pus, then the color of the turunda does not change, but if it is present, it becomes blue, green or bluish-green;
- Schiller-Pisarev test. It is aimed at identifying glycogen in the gums, a substance whose amount increases sharply during inflammation. The gums are lubricated with a modified Lugol's solution, after which the color is assessed. It changes from light brown to dark brown;
- radiography. In the image, the specialist determines how much the bone tissue is affected by the pathological process;
- swab from a dental pocket. The study is carried out to determine the causative agent of the disease that caused the inflammatory process;
- panoramic tomography. This procedure allows you to get a complete view of the affected jaw. The study is often carried out if generalized periodontitis is suspected.
Treatment methods
The treatment regimen and effectiveness depend on the severity of the pathological process. First, measures are taken to improve the condition of the gums themselves. For this purpose, local therapy is carried out, which includes:
- curettage or ultrasonic teeth cleaning. The procedure is necessary to remove tartar - supra- and subgingival. Ultrasound can also polish tooth enamel, which helps prevent future tartar formation;
- use of local antibacterial drugs. They come in a variety of gels that help suppress the development of bacteria in periodontal pockets. Examples of such drugs: Apident Active, Metrogyl Dent, Adepta;
- the use of anesthetic gels, such as Kamistad, Mundizal. They help get rid of sore gums;
- rinsing the mouth and washing periodontal pockets with antiseptic solutions such as Chlorhexidine and Miramistin;
- the use of special toothpastes with anti-inflammatory properties. They complement the main treatment prescribed by the doctor. Experts often recommend pastes such as Parodontax, Splat Active, Elmex Sensitive, Asepta.
Local anti-inflammatory therapy lasts for at least 10 days. Treatment is carried out twice a day: morning and evening. In parallel with the removal of tartar, caries is treated and non-viable teeth are removed. Even at the stage of drawing up a treatment plan, a decision may be made about the need for prosthetics. In this case, doctors prepare for this process, including tooth removal.
Sanitation of periodontal pockets can also be carried out using laser treatment. The laser is directed deep into the gums, which allows you to destroy pathogenic microorganisms, prevent bleeding and sterilize the oral cavity. This technique also stimulates recovery processes.
The general strengthening treatment regimen also includes various types of physiotherapy:
- balneotherapy,
- phototherapy,
- peloidotherapy,
- gum massage,
- UHF therapy,
- darsonvalization,
- electrophoresis,
- diathermocoagulation.
The main differences between acute and chronic periodontitis
Having considered the main characteristics of chronic and acute periodontitis, we can identify several main differences between these stages. Firstly, they differ in severity. Chronic periodontitis occurs slowly and often unnoticed by humans, while acute periodontitis is characterized by the suddenness and rapidity of damage to periodontal tissue.
Secondly, the factors that cause the disease vary significantly. Chronic periodontitis is caused mainly by general disturbances in the functioning of the body and bad habits, while the acute stage is provoked by mechanical damage to the teeth and gums due to injuries, certain types of dental diseases and improper installation of dentures.
Thirdly, the stages have different symptoms. If chronic periodontitis does not have a serious effect on the human body as a whole, then its acute form leads to intoxication, weakness, disrupting the usual course of life.
Fourthly, the localization of inflammation is somewhat different. In the chronic form, as a rule, the entire periodontium is affected to one degree or another, which is also typical for the acute non-purulent form. The acute purulent form is localized in a certain area of the oral cavity and leads to deepening of the periodontal pockets and significant swelling of the gums at the site of inflammation.
Fifthly, chronic and acute periodontitis require radically opposite measures of dental intervention. In the first case, regular preventative teeth cleaning at the dentist, treatment of the oral cavity with antiseptics to reduce the number of bacteria and relieve inflammation, physiotherapeutic procedures or treatment of periodontitis using the Vector apparatus are often sufficient. In the acute stage, it is often necessary not only to relieve inflammation, but also to remove a loose tooth, perform cavity surgery on the gums, or open the resulting fistulas and boils to remove pus. Patients often require consultation with an orthopedic dentist, who evaluates the possibility of installing dentures instead of extracted teeth.
Surgical intervention
When the depth of the periodontal pocket exceeds 5 mm, doctors decide on surgical treatment. In this case, a flap operation is performed - gingivectomy. It is carried out according to the following scheme:
- The gum is dissected, after which the gum flap in the area of the periodontal pocket is turned away.
- Next, the tooth root is cleaned and destroyed tissues and microorganisms are removed from the pocket.
- Then the tissues are washed with an antiseptic, after which the gum flap is returned to its place and sutures are applied.
The duration of the operation can be from 1 to 3 hours, it is performed under local anesthesia. During the process, the doctor can also straighten the bone tissue if inflammation has already spread to it. Depending on the nature of tissue damage, other operations may be performed:
- Gingivoplasty is a soft tissue transplantation. It is carried out when they are completely atrophied, when the tooth is completely exposed and visually becomes longer. To cover the defects, tissues from the palate are used. This helps stop the deepening of the periodontal pocket.
- Osteoplasty. It is carried out in case of destruction of bone tissue by inflammation, which can no longer hold the tooth in its place. During the operation, a graft made of bone tissue or synthetic material is used.
Another surgical method for treating periodontitis is splinting mobile teeth. This procedure allows you to keep them in place and save them from spontaneous removal. Splinting today is carried out in different ways:
- A horizontal bar and fiberglass tape are placed over several teeth. Then everything is filled with a light composite, as a result of which the dentition is connected.
- On the teeth, the upper part of which is previously ground down, crowns are put on, welded together.
- A clasp prosthesis is placed on the jaw, which allows you to evenly distribute the load on both the teeth and gums, and when installed on the upper row, on the upper palate.
Features of the initial stage of treatment of patients with severe periodontitis
T. V. Zakirov Ph.D., Associate Professor, Department of Pediatric Dentistry and Orthodontics, USMU
Periodontitis is one of the diseases with mild symptoms in the initial stages of its development. Typically, the only symptom of mild periodontitis is bleeding gums when brushing your teeth. Over time, this symptom disappears, and the disease does not manifest itself for a long time.
By the time severe periodontitis develops, the patient accumulates a whole complex of problems in the form of a pronounced loss of supporting-retaining periodontal tissues, pathological mobility and displacement of teeth, endo-periodontal lesions develop, periodontally altered occlusion, and occlusion of the dentition is disturbed [2, 7].
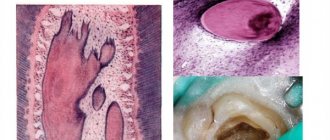
The condition is aggravated by the presence of concomitant somatic diseases in patients. These patients usually turn to the doctor at the stage of severe exacerbation of the inflammatory process in the periodontium with the presence of symptoms such as suppuration from periodontal pockets, sometimes abscess formation, severe tooth mobility, bad breath, etc. (Fig. 1, 2).
rice. 1. Oral cavity of a 30-year-old female patient with exacerbation of severe periodontitis. rice. 2. OPTG of the same patient, pronounced resorption of alveolar bone tissue.
The further prognosis for the entire human dental system often depends on the correct tactics of the dentist at this first stage. Unfortunately, in clinical practice, the choice of a doctor often takes one of the marginal positions: either total removal of teeth with subsequent problems with prosthetics, or, conversely, preservation of teeth in the absence of periodontal treatment as such. The situation is aggravated by the fact that the treatment of such patients requires the participation of almost all dental specialists, and the severity of the existing problems requires highly qualified doctors. In most cases, the first stage involves superficial cleaning of dental plaque.
Often this manipulation is performed by a clinic hygienist with secondary medical education. It should be noted that in the case of severe periodontitis, such tactics are unacceptable, because it inevitably leads to low effectiveness of the treatment, increases the likelihood of local and general complications, and makes it difficult to plan a further set of treatment measures. Patients, not seeing a significant improvement in the condition of their gums, lose confidence in the team of specialists and refuse recommended treatment measures (Fig. 3, 4). Therefore, knowledge of the features of managing patients with severe inflammatory periodontal diseases plays an extremely important role both in achieving clinical success at the initial stage of treatment and in planning further comprehensive dental rehabilitation.
rice. 3. Persistence of gum inflammation 1 month after professional hygiene in another clinic, right view. rice. 4. Oral cavity of the same patient, left view.
The first stage of treatment for patients with periodontal diseases should begin with a detailed conversation. During this period, the doctor must receive comprehensive information about the patient’s health status, medications he is taking, dietary habits and oral hygiene. Particular attention is paid to allergic diseases, diseases of the blood system with impaired coagulation, the speed of wound healing (regeneration can be suppressed due to diabetes mellitus, taking cytostatics, immunosuppressants, hormones; the risk of jaw necrosis is sharply increased when taking medications from the group of bisphosphonates, etc.). Despite the banality of this stage, it must be remembered that only the most detailed informing the doctor about the patient’s health status will help in the future to prevent the occurrence of serious complications in the form of unexpected bleeding, suppuration or extensive necrosis of periodontal tissue (Fig. 5).
When examining the patient, a periodontal card is filled out with a detailed indication of the depth of the periodontal pockets, the degree of gum recession, tooth mobility, the degree of furcation damage, etc. Hygienic and periodontal indices are assessed, as well as, if possible, the gum bleeding index. It is better to photograph the patient’s oral cavity before treatment and at the stages of complex therapy. Considering the constant increase in the legal literacy of patients, the increasing number of cases of defending their rights in court and the high cost of dental treatment, this stage is of particular importance.
The fact is that patients and doctors evaluate some results of treatment of moderate periodontitis completely differently. If the doctor pays attention to a decrease in the depth of periodontal pockets, a decrease in gum swelling and a decrease in exudation, then for the patient the leading symptom after the treatment will be exposure of the roots, loosening of the teeth and increased sensitivity (Fig. 6, 7).
rice. 5. Necrosis of the gums after professional hygiene due to 10 years of taking methotrexate. rice. 6. View of the gums before treatment in severe aggressive periodontitis. rice. 7. Generalized gum recession 1 month after the first stage of treatment.
Naturally, these symptoms are assessed sharply negatively by patients, so the patient should be warned about their development in advance when signing informed consent. In this case, emphasis should be placed on the temporary nature of the changes that occur. Increased sensitivity gradually disappears, pathological mobility of teeth also decreases, and gingival papillae are fully or partially restored while maintaining the distance from the contact point to the alveolar ridge within 5-7 mm [8]. In severe periodontitis, these changes are irreversible, but the doctor must focus on their cause (advanced periodontitis and loss of a large amount of tissue as a result of a long-term inflammatory process in the periodontium), as well as on the possibility of completely eliminating or leveling these symptoms at subsequent stages of treatment (splinting teeth, restoration, etc.). In other words, forewarned means forearmed.
The actual treatment of a patient with severe periodontitis must begin with empirical antibiotic therapy. The pronounced stage of inflammatory periodontal disease is characterized by deep massive invasion of aggressive anaerobic bacteria not only into the tissue of the periodontal complex and other organs and tissues of the oral cavity (for example, periodontal pathogenic microorganisms are found in the folds of the tongue, tonsil crypts, epithelial cells of the mucous membrane), but also in remote regions of the human body. body (endocardium, atherosclerotic vascular plaques, etc.).
In addition, after professional hygiene in severe periodontitis, a fairly large number of microorganisms are released into the blood - the phenomenon of transient bacteremia occurs [3]. And if in most patients this is accompanied by a feeling of weakness, malaise and a slight increase in body temperature, then in patients at risk (prosthetic heart valves and joints, congenital or acquired endocardial defects, etc.) this can lead to such serious complications as bacterial endocarditis or even sepsis [4].
Therefore, only systemic antibiotic therapy will suppress the majority of pathogenic microbes in the biofilm on the root surface, significantly increase the effectiveness of treatment, improve the healing period after dental intervention, and prevent the occurrence of local and general complications [6].
The drugs of choice include antibiotics such as Tsifran ST (a combination of ciprofloxacin and tinidazole) 1 tablet. 2 times a day, amoxiclav (amoxicillin and clavulanic acid) 375 mg, 1 tablet. 3 times a day, doxycycline 100 mg 2 times a day. Usually, at the stage of exacerbation, it is enough to prescribe drugs for 5-7 days. For patients wary of antibiotic therapy, more modern once-daily medications can be recommended, such as sumamed (azithromycin) 500 mg for 3 days or avelox (moxifloxacin) 400 mg for 5 days. In this case, the minimum inhibitory concentration of the antibacterial drug will be maintained in the patient’s body for a week.
Antibiotic therapy should be started 1-2 days before professional oral hygiene. Key point: the main treatment of periodontal pockets, even if it is divided into several stages, should involve taking antibiotics. It is important to focus the patient’s attention on the need to take an antibiotic; to increase motivation, you can show him suppuration from the pockets by applying finger pressure to the gums.
Of course, antibiotic therapy is a serious medical intervention in the human body, so it must be carried out in compliance with all the basic requirements of chemotherapy, taking into account the patient’s health status, indications and contraindications, and under the constant supervision of a physician. To minimize the side effects of antibacterial drugs, it is necessary to prescribe in parallel the administration of eubiotics for 2 weeks (Linex, Bifiform, Acipol, etc.).
It is better to carry out the treatment of periodontal pockets in 2 visits, separately for the upper and lower jaws, although under certain conditions (small number of teeth, remote place of residence of the patient) all the work can be carried out in one visit. Before use, the patient should rinse the mouth with an antiseptic, for example 0.2% chlorhexidine, which will reduce the contamination of the bacterial aerosol generated when using ultrasonic devices.
A prerequisite for effective pocket work in the vast majority of patients is adequate pain relief. A priori, it is impossible to treat the root surfaces to the full depth when using topical anesthesia. To increase the effectiveness of anesthesia in the lateral areas of the lower jaw, anesthetic injections are carried out not in the area of the transitional fold, but in the area of the attached gum. This promotes better deposition of the anesthetic and its penetration through the cortical plate of the jaw.
Considering the number of injections, it is necessary to periodically replace the needle to reduce trauma and pain when puncturing the mucous membrane. In the case of particularly massive jaws and significant destruction of bone tissue in the area of the interdental septa, conduction anesthesia may be the method of choice.
Treatment of periodontal pockets at the first stage of treatment of periodontitis should include not only the removal of dental plaque above and below the gum, but also smoothing the surface of the roots, correction of overhanging fillings in contact areas, removal of granulations, rinsing with antiseptics and, if necessary, in especially problem areas, should be completed by applying local antibacterial drugs in addition to systemic antibiotic therapy. It should be noted that, contrary to the opinion of many doctors, removal of deposits is not the only goal of this procedure. In case of aggressive periodontitis, for example, hard dental deposits may be completely absent, however, despite this, the pathological process is characterized by a highly pronounced destructive effect on periodontal tissue, rapid progression and low effectiveness of treatment [1].
There are often cases when patients undergo vector therapy 4 times a year, but this does not lead to any significant improvement in the condition, and sometimes (for example, with simultaneous orthodontic movement of teeth) it even ends catastrophically (Fig. 8, 9).
rice. 8. Severe inflammation of the gums with ineffective regular vector therapy. rice. 9. Progressive bone resorption as a result of orthodontic treatment.
A much more important goal of working in periodontal pockets is to remove a large amount of inflammatory granulation tissue, suppress the activity of periodontopathogenic microflora and shift the biocenosis of periodontal pockets towards less aggressive saprophytic species. It is necessary to begin work with ultrasonic devices, which remove the bulk of dental plaque. Without dwelling on the principles of operation of these devices, it should be noted that the treatment should be carried out to the entire depth of the periodontal pocket. In this case, partial separation of the granulation tissue occurs, and it is then easier to remove it with hand instruments. The mandatory set of tools when treating pockets includes not only ultrasonic devices, but also periodontal burs and curettes (Fig. 10, 11).
rice. 10. Burs for working in periodontal pockets. rice. 11. Comparison of the working parts of the scaler, universal curette and Gracie curette.
Without hand tools, periodontal pockets are not treated all over the world, although the choice of a specific set of tools remains at the discretion of the specialist [5]. The main characteristics of such instruments are a rounded, non-aggressive tip (for working in the subgingival area) and sharp working edges. Today there are enough opportunities for regular sharpening of curettes, which can be carried out both in specialized centers and independently in a dental clinic (Fig. 12, 13).
rice. 12. Device for sharpening periodontal curettes. rice. 13. Checking the sharpness of hand tools.
When working with hand instruments, involuntary dissection of the gingival papillae in the interdental area is possible. In most cases, this does not require suturing: in conditions where the mucoperiosteal flap is not peeled off, the papillae, after the end of the procedure and the onset of hemostasis, take their original position and the postoperative period proceeds without any complications. We also do not recommend applying periodontal dressings. In conditions of inflammation, they only interfere with the healing process - they compress the swollen gum tissue, impede the free evacuation of the contents of periodontal pockets, and again create conditions for the growth of anaerobic microflora.
Despite the fact that modern devices sometimes have built-in methods for detecting hard dental deposits, the best method for diagnosing them remains probing the root surface with a periodontal probe.
Elements of curettage require certain skills, and this procedure can be carried out by a doctor with a higher medical education, regardless of his profile - this can be done either by a therapist or dental surgeon specializing in the treatment of periodontal diseases, or by a periodontist at a clinic (let me remind you that the specialty There is no periodontist in Russia). Due to the increased invasiveness, it is unacceptable to entrust this treatment to a hygienist: this will not only be ineffective, but in some cases it is dangerous for the health and life of the patient.
The result of a correctly carried out first stage of periodontitis treatment is a significant improvement in the condition of periodontal tissues. Regardless of the severity of the disease, the gums acquire a pale pink color, active exudation and suppuration from periodontal pockets stop, tooth mobility decreases, and bad breath disappears (Fig. 14, 15).
rice. 14. Severe periodontitis in the acute stage in a patient. rice. 15. View 1 month after the initial stage of treatment, relief of inflammation.
Patients usually note an improvement in their condition. It should be noted that sometimes, with particularly deep periodontal pockets and severe bleeding gums, it is not possible to carry out full treatment in one visit. In this case, the remnants of dental plaque and granulations can be removed after 3-4 weeks under conditions of better visibility, after the inflammatory phenomena have subsided. The only condition is that it is necessary to timely assess the severity of the disease, the amount of deposits on the teeth and warn the patient about the need for a two-stage procedure.
After a month, you can take repeated photographs of the oral cavity and gather a consultation of specialists to develop a further treatment plan. Obviously, in conditions of stopping the acute inflammatory process in the periodontium, it is easier for doctors to assess the current clinical situation, the true mobility of the teeth, and the resulting gum recession. From experience, it can be noted that even with further surgical treatment using modern osteoplastic materials and membranes, recession, if increased, is very slight, and in some cases the degree of root exposure can even be reduced by carrying out orthodontic treatment or bringing the contact point closer to the gingival papilla (Fig. 16, 17).
rice. 16. Severe gum recession with abnormal position of teeth against the background of periodontitis. rice. 17. Reduction of gum recession after orthodontic treatment.
Only when remission of the inflammatory process in the periodontium is achieved can a correct, informed decision be made on further therapeutic measures [9]. Thus, an orthodontist will be able to assess the possibility of moving teeth, and an orthopedic dentist will be able to assess the possibility of using teeth as a support for fixed dentures. Sometimes the effectiveness of deep cleaning of the gums is so high that there is no need for surgical interventions with flaps and the time for complex rehabilitation of the human dental system is significantly reduced. The effectiveness of the following stages of treatment also increases.
For example, even in the case of a surgical intervention with a flap, the surgeon will not spend additional time removing dental plaque, which, in conditions of generalized lesions, will certainly significantly reduce the operation time. Regardless of the preservation of the tooth, the procedure for regenerating bone tissue or preserving the volume of the socket will be more effective, since bone formation will occur in the absence of an inflammatory process, the retaining function of the sutures will also increase due to the restoration of the original gum density (Fig. 18-22).
rice. 18. Abscess formation in the area of the 11th tooth with severe periodontitis. rice. 19. View 1 month after professional hygiene. rice. 20. View 5 months after the removal of teeth 12 and 11 with osteoplasty of the sockets. rice. 21. View 2 years after prosthetics on implants. rice. 22. Look when smiling.
Thus, a correctly carried out first stage of treatment of moderate periodontitis creates conditions for increasing the effectiveness of complex dental rehabilitation, reduces the likelihood of complications and increases patient confidence in the team of specialists.
Information about the author Zakirov Taras Valerievich, Ph.D., Associate Professor of the Department of Pediatric Dentistry and Orthodontics, USMU (Ekaterinburg)
Zakirov TV, Ph.D., Assistant, Department of Pediatric Dentistry and Orthodontics, UGMA
Features of the initial stage of treatment of patients with severe periodontitis
Annotation. Periodontitis is one of the diseases with mild symptoms in the initial stages of its development. Typically, the only symptom of mild periodontitis is bleeding gums when brushing your teeth. Over time, this symptom disappears, and the disease does not manifest itself for a long time.
By the time severe periodontitis develops, the patient accumulates a whole complex of problems in the form of a pronounced loss of supporting-retaining periodontal tissues, pathological mobility and displacement of teeth, endo-periodontal lesions develop, periodontally altered occlusion, and occlusion of the dentition is disturbed.
Annotation. Periodontitis is one of the diseases with mild symptoms at the initial stages of its development. Usually the only symptom of mild periodontitis is bleeding gums when brushing your teeth. Over time, this symptom disappears, and for a long time the disease does not manifest itself.
By the time severe periodontitis develops, the patient has accumulated a whole range of problems in the form of pronounced loss of periodontal supporting and retaining tissues, pathological mobility and tooth dislocation, endoperiodontal lesions, periodontal malocclusion develop, and occlusion of the dentition is impaired.
Key words: periodontitis, empirical antibiotic therapy, periodontal pocket, granulation tissue
Keywords: periodontitis, empirical antibiotic therapy, periodontal pocket, granulation tissue
Indications
Vitamins A and C are especially important for patients with periodontitis. It is necessary to include more fruits, vegetables and herbs in the diet. At an early stage, when the teeth are not yet loosened, you can eat the fruits in solid form. This will ensure the necessary load on the dental system. It is necessary to chew on both sides, and not just one, so that all areas of the teeth work actively. It is useful to include the following products in the menu:
- seafood;
- apples;
- Bell pepper;
- avocado;
- dill, parsley;
- black currant berries;
- carrot;
- peanut;
- citrus.
The diet must include dairy products, which are a source of calcium. The patient needs to consume more milk, sour cream, cottage cheese, and different types of cheese. Vitamin A, which promotes epithelial regeneration, is found in pork and beef liver, pumpkin, apricots, broccoli and spinach. Zinc, which is present in lentils, peas, and seafood, is useful for bone tissue. If you have periodontal disease, it is better to drink green tea or natural juices.
Advantages of treatment at JSC "Medicine"
By contacting JSC “Medicine” (clinic of Academician Roitberg), you can be sure that the examination will be carried out as completely as possible and exclusively using high-precision equipment. From the first contact to receiving test results, no more than a day passes. Also, each patient of the clinic is provided with:
- an accompanying person to move around the clinic;
- personal physician-supervisor who will monitor the progress of diagnostics and treatment processes;
- written recommendations regarding treatment and all necessary information regarding prescribed medications.
At the clinic of JSC "Medicine" you will not waste your personal time in line. Our medical center provides services at an international level of quality, and if controversial issues arise, the administration is always ready to consider any requests.
Preventive measures
To prevent the development of localized periodontitis, the following measures are recommended:
- choose the right toothbrush, toothpaste and mouthwash, maintain oral hygiene and floss after meals;
- create a correct and balanced menu, take vitamins;
- exercise to strengthen your immune system;
- undergo a preventive examination at the dentist every six months, and if symptoms of the disease occur, consult a doctor in a timely manner. Do not trigger any pathologies and disorders in the body;
- try to reduce your stress level - distract yourself with walks, massages and other pleasant and useful rest.
These measures will help prevent the development of not only dental, but also other diseases that affect the condition of the oral cavity.