Publication date: June 28, 2022.
Information on this page was updated on October 15, 2021.
Mesial occlusion is recognized by researchers and practicing orthodontists as one of the rarest and most difficult dental pathologies to treat.
Mesial occlusion or progeny is a type of malocclusion in which the lower jaw protrudes forward relative to the upper jaw. The lower incisors overlap the upper ones or form a reverse sagittal fissure - the space between the front and lower front teeth.
Reverse incisal overlap
Reverse incisal overlap on CBCT image
How to determine mesial bite?
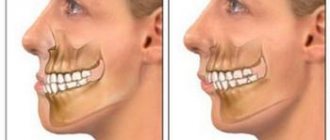
- By the face. Mesial occlusion can be determined by the structure of the face even without looking at the smile. The profile is concave - the middle third of the face falls back slightly, especially relative to the lower third. The chin protrudes forward and looks massive and disproportionate to the face and upper jaw. At the same time, the lower lip looks thicker, and the upper lip sinks. The facial expression seems angry.
- By posture. The temporomandibular joint is directly connected to the spine, so its malposition (as a result of malocclusion) affects the posture and balance of the entire body. Those with complex forms of mesial occlusion are characterized by a slight deviation of the body backwards. If you draw a straight line through the entire body in profile, the head will be tilted slightly back, and the pelvic bones will be pushed forward.
Concave profile with mesial bite
Poor posture with mesial occlusion - By smile and teeth. The clinical situation in which the lower incisors are in front of the upper ones is called reverse incisal overlap. This is the most characteristic intraoral sign of progeny. It is also characterized by: gaps between the teeth, dystopia (improper position) of the teeth, tilting of the lower teeth into the oral cavity.
What happens if you don't correct your bite?
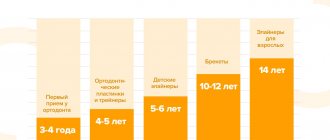
It is recommended to correct prognathia of the upper jaw in a child before the age of 14, after which it may be too late. If treatment is ignored, an adult may experience the following complications:
- pathological occlusion or violation of aesthetic facial features - protrusion of the jaw and a reduced shape of the chin provoke complexes associated with appearance, which causes a decrease in self-esteem;
- dysfunction of chewing and swallowing - improper closure of teeth requires a person to put 30% more effort into chewing food compared to the norm;
- diction disorders - the appearance of speech therapy problems.
Also, people with prognathia have an increased risk of developing dental diseases - caries, pulpitis, gingivitis and periodontitis. This is due to a high degree of load on individual areas of the periodontium and teeth.
Types of mesial occlusion
By form:
- Dentoalveolar form. Malocclusion as a result of incorrect position of the teeth.
- Gnathic or skeletal form is an abnormal bite formed by a pathology of jaw development.
A more complex form of malocclusion, sometimes requiring surgical intervention. Often, clinical cases of mesial malocclusion combine both forms - incorrectly positioned teeth and abnormal jaw sizes.
For reasons of occurrence:
- Congenital abnormal jaw sizes: macrognathia of the lower jaw - a large or elongated lower jaw; micrognathia of the upper jaw - underdeveloped, small upper jaw.
- Prognathia of the lower jaw is a forced position when individual teeth interfere with the normal closure of the jaws and jaw growth. This type of bite occurs in children on their baby teeth due to fangs that cling to the lower teeth and prevent the lower jaw from taking a normal position.
- Retrogression of the upper jaw is the posterior position of the upper jaw relative to the proportions of the face. Unlike micrognathia, in this case the jaw is of normal size, but incorrectly positioned.
- Abnormal tooth sizes: macrodentia - large teeth on the lower jaw, microdentia - small teeth on the upper jaw.
Classification
Now the authors have identified a number of classifications of occlusion. Depending on this, the type of treatment and preventive measures may vary greatly.
According to the degree of morphological changes
Depending on this, the following forms of the disease are distinguished:
- Gnathic. It is formed against the background of a violation of the development of facial bones. In particular, it occurs as a result of a disturbed location or size of the jaws.
- Dentoalveolar . Occurs when the buds of the teeth are incorrect, as well as a significant difference in the size of the jaws. Sometimes the disease can appear against the background of a violation of the shape of the process of the upper jaw.
Some authors identify a mixed form of the disease, in which signs of both forms are noted.
Is it possible and how to straighten teeth at home without the participation of a specialist?
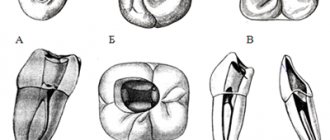
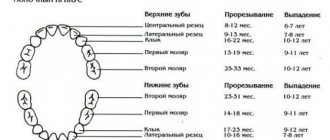
Visit here to learn more about the stages of permanent dentition formation.
At this address https://orto-info.ru/zubocheliustnye-anomalii/okklyuzii/pri-smennom-prikuse.html we will discuss what difficulties may arise when forming a mixed bite.
By localization
In this case, experts distinguish partial and general forms of the disease . For the general type, violation of the location of both lateral and frontal teeth.
In case of partial violation, only the contact of the anterior units suffers.
According to etiological factor
According to the etiology, progeny can be true or false:
- True is a condition in which both the front and lateral teeth are positioned incorrectly, and with central occlusion, a space is formed between the front elements.
This form of the disease is characterized by severe disruption of the jaws. Thus, patients cannot bite and chew food normally, and the jaw itself protrudes forward quite strongly, which causes severe psychological and aesthetic discomfort. - For false progeny, only a few front teeth are in the wrong position. Basically, this form of the disease is observed in older people, or against the background of improper surgical treatment.
- Some authors also highlight forced progenic occlusion. This type of disease occurs when there are temporary bumps in the lower jaw.
At the same time, the dentition remains normal. At rest, no manifestations of pathology are visible, however, when the teeth close together, signs of a progenic bite appear.
Causes of mesial bite
In the early stages of development:
- Heredity - congenital abnormal structure of the skull and facial bones. It is transmitted genetically, sometimes depending on ethnicity. The likelihood of mesial occlusion in the Mongoloid race is higher than in Caucasians.
- Mother's illnesses during pregnancy, unfavorable external environment, lack of nutrients during intrauterine development.
- Incorrect breastfeeding.
- Macroglossia is an increased size of the tongue.
- Childhood diseases (rickets, endocrine gland disorders)
- Bad habits: sucking the upper lip, finger.
- Short frenulum of the tongue.
During the period of milk and permanent teeth:
- Impaired wear of baby teeth, as a result of which the teeth (usually fangs) interfere with the normal closure of the upper and lower jaws. When closing, the lower jaw slips and takes a forced position in front.
- Late eruption or early loss of teeth in the upper jaw.
- Supernumerary teeth on the lower jaw.
- Incorrect body position: lowering the head on the chest during sleep, resting the chin with the hand in a sitting position.
Prognathia: causes of occurrence
Distal bite, as this defect is also called, is most often congenital, hereditary in nature - the risk of developing such an anomaly is higher in people whose parents or grandparents also suffered from bite problems. But there are several other reasons why a child develops prognathia:
- pathologies of intrauterine development of the fetus;
- pathologies of postnatal development;
- improper nasal breathing in childhood;
- incorrect method of artificial feeding, when the baby makes almost no effort to suck milk from the nipple - the lack of load on the masticatory muscles leads to disruption of the development of the bite;
- too early loss of baby teeth, especially canines;
- a complication after rickets - a disease of infants and young children, which leads to impaired bone formation and insufficient mineralization due to vitamin D deficiency.
Consequences of mesial occlusion
First of all, mesial occlusion disrupts external aesthetics. A disproportionate face reveals an incorrect bite even if the person is not smiling. The facial expression seems stern and angry.
Irregular incisal overlap and gaps between the front teeth greatly complicate the chewing process. The front teeth wear against each other, and the entire chewing load is redistributed between several teeth, which decay faster and are more susceptible to caries due to constant work. When teeth are lost as a result of malocclusion, implantation and prosthetics are complicated - there may not be enough space for adequate restoration of teeth.
If the upper incisors, as a result of reverse overlap, reach the mucous membrane of the lower jaw, then a chronic injury occurs at the site of contact. It leads to bacterial growth, periodontitis, recessions and an increased risk of cancer.
Improper dental alignment or jaw structure directly affects the temporomandibular joint. The result of incorrect position of the joint is clicking, pain when opening the mouth or chewing food, headaches, dystrophy and jamming (freezing in one position) of the joint.
Complications with mesial occlusion
If the mesial bite is not corrected, then in the future this leads to the following complications:
- Psychological problems . They arise due to irregular facial shapes. With such a defect, a person begins to be embarrassed about his appearance and feels insecure.
- Tooth decay . Due to the disruption of teeth closure, hard tissues are destroyed faster. With a mesial bite, only some teeth bear the main load. This speeds up their destruction.
- Disorders of the digestive tract . Violation of the chewing process leads to the fact that poorly processed food (relatively large pieces of food) enters the stomach. This impairs the functioning of the gastrointestinal tract, contributing to the development of gastritis and dyspepsia.
- Disorders of the temporomandibular joint . When moving the jaws, clicks are noticeable. Subsequently, pain occurs. In severe cases, the person is unable to open or close their mouth.
Diagnostics
To draw up a complete clinical picture and treatment plan, you need high-quality diagnostic data of several types:
- Visual examination of teeth and face by an orthodontist. Usually occurs at the first consultation. The doctor evaluates the position, size and condition of the teeth. If necessary, refers to additional specialists.
- Assessment of jaw position and size using CBCT. Only a 3D image of the entire skull will give the doctor an accurate idea of how the jaws are positioned relative to each other and the condition of the temporomandibular joint. Based on these data, a plan for moving the teeth is drawn up, and the need for surgical intervention or additional treatment of joint dysfunction is assessed.
- Assessing the position, relationship and closure of teeth using impressions.
- A detailed photo protocol for drawing up a treatment plan and further monitoring the dynamics of treatment.
Treatment at the CIS clinic, Kyiv
At the Center of Israeli Dentistry, treatment of mesial occlusion is based on three pillars:
- Diagnostics. The most important stage for understanding further treatment strategy. To clarify the diagnosis, we use modern types of tomography, including three-dimensional images. It is noteworthy that the examination is carried out regularly and during treatment to monitor the result.
- Modern orthodontics . We often begin treatment by correcting the patient's posture, as this has a significant impact on the jaws. Only after this we begin treatment with modern braces and other orthodontic structures.
- Honesty . We never offer patients knowingly ineffective methods of bite correction. If during the diagnostic procedures it becomes clear that the patient needs surgical intervention, the orthodontist at the CIS clinic will speak directly about this.
Correction of mesial bite
Treatment
Treatment methods for mesial malocclusion depend on the patient’s age and the shape of the malocclusion (skeletal or alveolar). Earlier treatment is usually faster and more effective because the jaws, teeth and alveolar bone tissue are in the growth phase.
Treatment in milk and mixed dentition
When diagnosing mesial occlusion in a child with primary or mixed dentition, first of all, it is necessary to exclude factors that aggravate the pathology:
- bad habits. Special jaw appliances will help make it easier to wean yourself from a bad habit and adapt to the correct position of the jaws.
- improper swallowing or mouth breathing. To eliminate breathing problems, you will need to consult an ENT doctor.
- forced position of the jaw due to interfering tubercles or cutting edges of individual teeth. In this case, the teeth are ground to a safe extent for normal closure.
If the lower jaw is shifted forward slightly, then massage of the alveolar process (the place where the teeth grow) from the side of the palate in the anterior part of the upper dentition is indicated for correction. The general position of the jaw is corrected with removable devices.
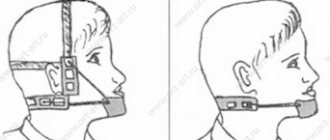
In case of deep incisal overjet, the Brückle apparatus is used in the mixed dentition. It moves the upper teeth forward, and the bite block helps to release the bite on the anterior teeth.
Jaw development can be further hampered by pressure from the lips, tongue, and cheeks on the alveolar bone and teeth. The type 3 Frenkel function regulator normalizes the position and relationship of the teeth, tongue and cheeks.
Bruckle apparatus
Frenkel apparatus type 3
Studies show that it is impossible to restrain the growth of the lower jaw, therefore, in the primary and mixed dentition, orthodontic treatment is focused on stimulating the growth of the upper jaw. To do this, a partial bracket system “4+2” is installed on the permanent incisors and first molars. The action of braces helps to expand and lengthen the upper jaw.
Partial bracket system for mesial occlusion"
Treatment in permanent dentition of dentoalveolar form
In the dentoalveolar form, the mesial bite is formed due to the incorrect position of the teeth. To correct it, it is enough to install a braces system. Treatment is carried out with the mandatory use of intermaxillary traction - elastics, which help to pull the lower dentition back. In case of severe anomaly, the lower eighth teeth (wisdom teeth) are removed, and mini-screws are connected to extend the dentition. Mini-screws or micro-implants are small screws that become absolute support.
Treatment of gnathic permanent dentition
The skeletal form of the bite, that is, fixing the bite at the level of the skull bones, requires additional surgical intervention. An orthognathic surgeon corrects the size and position of the jaws after installing braces and adjusting the position of the teeth. After the operation, the orthodontist details the position of the teeth for a perfect smile.
Prevention
The development of mesial malocclusion can be prevented by following these recommendations:
- eliminate improper feeding, choose the correct shape and size of the nipple in accordance with the age of the child;
- promptly transfer the child to solid food, which stimulates the chewing muscles;
- monitor oral hygiene;
- Treat dental and oral diseases in a timely manner;
- wean your child from bad habits - sucking a finger, objects, biting the upper lip and others;
- Avoid improper mouth breathing.
The above measures do not provide a 100% guarantee, but they significantly reduce the likelihood of developing a mesial bite.