Various types of fractures lead in frequency among injuries to permanent teeth; the central incisors of the upper jaw are most often damaged. As a percentage, fractures account for about 67% of all types of injuries to permanent teeth; for baby teeth this figure is much lower - about 7%.
The success of treating dental fractures directly depends on the speed at which the patient seeks dental care; in some cases, this must be done in the first hours after the injury occurs.
What is
Not everyone knows about a tooth fracture, but dentists encounter this problem quite often. Many fractures occur in children, boxers, stuntmen, and active sports enthusiasts. Another common option is accidents when a fracture is caused by accidental mechanical damage. It often occurs during an accident or fight.
As is the case with various parts of the body, a fracture negatively affects the anatomy and natural shape of the tooth.
A tooth fracture is a violation of the integrity of dental tissue (one or more of its layers) down to the tooth root. In most cases, the upper front teeth, in particular the central incisors, are affected. A fracture of the alveolar process, root or crown may also occur.
Possible complications
A fracture of a baby tooth in a child usually does not lead to complications, as it is accompanied by the removal of a temporary tooth and subsequent observation.
In adults, trauma to a permanent tooth can lead to its loss and a long recovery process. Delayed contact with the dentist leads to:
- To an abscess of the maxillofacial area.
- The formation of phlegmon is a purulent-necrotic inflammation that can lead to sepsis or meningitis.
- Tooth loosening and loss.
- Acute pulpitis.
- Pulp atrophy, that is, its replacement with connective tissue.
- Inflammation of the periosteum (periostitis).
Long-term consequences of injury include root resorption, that is, resorption of the bone tissue surrounding the tooth. This phenomenon is normally observed in children when changing baby teeth.
If, after a minor injury, a person does not go to the dentist, then it should be taken into account that the integrity of the tooth may be compromised. A crack or break is not always noticeable outwardly, and the painful syndrome is mild. In this case, the tooth may not withstand normal chewing load. This can lead to a complete fracture.
Common Causes
In addition to the factors mentioned above, it is also worth noting unqualified treatment. For example, when removing a lower jaw tooth with forceps, you can damage one of the upper teeth with the instrument. If a tooth is weakened by various diseases or is in poor condition, the likelihood of a fracture is very high. Of course, such cases are very rare, but they do happen. Another reason for a fracture is an error at the stage of selecting the size of the holes in the pins. It is important to note that the lack of treatment for caries also negatively affects the condition of the enamel, as a result of which sometimes eating solid foods can provoke a crown fracture. Do not forget about the anatomical features of the jaw. If its structure has certain defects, the pressure will be distributed incorrectly.
Causes of fractures
Tooth fractures occur when:
- a strong blow to the tooth during a game, a fall, an accident, or doing any work;
- contact of solid food with a tooth with a carious cavity or with a previously treated tooth with large fillings;
- presence of bad habits (crunching nuts in shells, opening beer bottles with teeth);
- abnormal bite;
- hitting the antagonist tooth with dental forceps when removing a tooth on the opposite jaw.
A tooth fracture can occur in any part of the tooth; In direction, fractures are longitudinal, oblique and transverse.
Diagnostics
If a tooth is fractured, you must consult a dentist. Of course, if the problem does not cause discomfort, which occurs in rare cases, there is no need to rush. But delay can cause even more serious damage, resulting in the tooth having to be removed. Fracture of the anterior elements of the dentition has an extremely negative effect on the beauty of the smile.
A specialist can easily diagnose a tooth fracture. You just need to establish the extent of the fracture and understand whether the remains of the tooth can be saved. To do this, an x-ray is taken, with which the doctor checks for displacement, damage to the root, adjacent tissues and the direction of the fracture. The specialist examines the injured area, analyzes the presence of external damage, swelling, and changes in the color of the enamel. The latter may be a sign of soft tissue necrosis or damage to the neurovascular bundle and filling of the dentinal tubules with blood.
If during percussion a person experiences painful sensations in the damaged tooth and nearby elements of the dentition, this may be a sign of injury to the periodontal and periapical tissues or tooth dislocation. Electroodontometric diagnostics may also be necessary, with which the doctor checks the viability of the pulp in the event of a serious fracture, so that in some cases it can be preserved.
Acute dental trauma. Classification. Terminology. Diagnostics
N.V. Gnali MD, Professor, Head of the Department of Pediatric Dentistry, SSMA, Chief Physician of the MAXIMA Dental Clinic
D. V. Rogatskin , radiologist, ORTOS LLC
The main purpose of clinical classification, in addition to systematizing knowledge, is to help the doctor make a diagnosis, plan treatment, and predict results. Assessing the existing classifications of acute dental trauma (hereinafter referred to as ADT), one can note two trends in their compilation: the first is the desire to describe all types of ADT, the condition of the pulp, periodontium, possible complications, the second is the desire to simplify the classification by including the most common injuries.
The format of the article does not allow us to present the mentioned classifications in full; we will limit ourselves to only a few comments. The disadvantage of the classification proposed by the Bulgarian authors Sl. Davydov and Z. Peneva (1964), in our opinion, is the inclusion of a section “Traumatic periodontitis” in it, which does not correspond to the generally accepted classification of periodontitis, which distinguishes acute, chronic periodontitis and chronic periodontitis in the acute stage.
The term “traumatic” indicates only the cause of periodontitis, and not its course. The nosological forms introduced by the authors: “Loosening of teeth without dislocation”, “Rupture of the neurovascular bundle without loosening of teeth” are not types of injury, but its consequences.
In the classification developed by V.F. Vasilevskaya (1970), types of crown fractures in the area of enamel and dentin are distinguished based on the transillumination of the pulp, which seems to us rather arbitrary due to the same treatment for this pathology. In our opinion, it is inappropriate to introduce into the “Combined trauma” section simultaneous, but different in form, injuries to two or three teeth of one patient. In addition, the classification does not take into account all types of combined tooth damage.
It is extremely difficult to use in practice the classifications proposed by G. M. Ivashchenko (1963) and A. M. Konstantinov (1985), due to the unsystematic and incomplete listing of nosological forms of injuries. Thus, G. M. Ivashchenko did not include in the working classification the definition of the type and level of the tooth fracture line, which is necessary to know when planning treatment. A. M. Konstantinov uses not a clinical, but a metric assessment of damage - “Fracture of 1/3 or 2/3 crown.”
This is quite difficult to determine due to the different size, shape and location of the broken part; in addition, this information is not decisive when planning treatment. It is unacceptable, in our opinion, to distinguish between “complicated” and “uncomplicated” root fractures, since this involves combining the injury as such with its consequences.
One of the latest is the classification developed by V.V. Roginsky (1987). In our opinion, there is no reason to complicate the classification by indicating the degree of formation of the root of the injured tooth. You should also not include tooth contusion in the classification as a nosological form, since it is impossible to diagnose it on the basis of the signs proposed by the author.
Pulp necrosis, identified by the author (class I-II, type 3), is a consequence of trauma, and not a nosological form.
In our country, the best known classification is N.M. Chuprynina, published in the latest edition in 1993 (Chuprynina N.M., Volozhin A.I., Ginali N.V. Dental trauma, 1993). In this classification, in particular, dislocations with displacement of a tooth towards the adjacent one and rotation of the tooth along the axis are considered separately.
In our opinion, a tooth physically cannot rotate along its axis, much less move towards the adjacent one, without preliminary extrusion, which in this classification is also considered as an independent form of dislocation. In addition, there is the author’s interpretation of the concepts of “combined” and “combined” trauma, which contradicts general medical concepts in this area. And finally, the category “trauma of the germ” is highlighted.
Since the germ is not a full-fledged tooth and cannot be directly injured, consideration of this nosology in the classification of acute dental trauma is unjustified.
The WHO classification is known, which identifies 8 classes of HTA:
- Class 1: Tooth contusion with minor structural damage.
- Class 2. Uncomplicated fracture of the tooth crown.
- Class 3. Complicated fracture of the tooth crown.
- Class 4. Complete fracture of the tooth crown.
- Class 5. Coronal-root longitudinal fracture.
- Class 6. Tooth root fracture.
- Class 7. Tooth dislocation (incomplete).
- Class 8. Complete tooth dislocation.
The classification created by Jacobsen (1981) is simple and accessible to practitioners. However, the classification of Andreason et all (Andreason JO, Andreason F., Andreason L., Textbook and Color Atlas of the Traumatic Injuries to the Teeth, 2007) is most widespread abroad:
- Crown fracture.
- Fracture within the enamel.
- Fracture within enamel and dentin.
- A simple crown-root fracture within the dentine enamel and cementum.
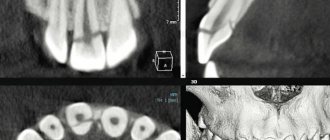
- Fracture within the enamel, dentin and pulp (Fig. 1).
- Complete coronocoronal fracture within the enamel, dentin, pulp and cementum (Fig. 2).
Rice. 1. CT, visualization of tooth 11, MPR; fracture within the enamel, dentin and pulp.
Rice. 2. CT, visualization of tooth 22, sagittal reformat and volumetric rendering; Complete coronal-coronal fracture within the enamel, dentin, pulp and cementum.
- Root fracture.
- Root fracture within cementum, dentin and pulp (Fig. 3).
Rice. 3. CT, visualization of tooth 21, MPR; root fracture within the cementum, dentin and pulp.
- Damage to periodontal tissue.
- Injury.
- Subluxation (subluxation).
- Dislocation with displacement (lateral luxation, Fig. 4, 5).
- Intrusion (impacted dislocation).
- Extrusion (dislocation with extension from the socket, Fig. 6).
- Complete dislocation (avulsion, Fig. 4).
Rice. 4. CT, visualization of tooth 21, MPR; dislocation with displacement (lateral luxation) of tooth 21, complete dislocation (avulsion) of tooth 22.
Rice. 5. CT, visualization of tooth 21, MPR; dislocation with displacement (lateral luxation) of a fragment of tooth 21 (sagittal reformat) and tooth 11 (coronal reformat), fracture of the alveolar process in the area of the alveolar part of the palatal cortical plate (axial reformat).
Rice. 6. CT, visualization of tooth 42, MPR; dislocation with displacement, extrusion (dislocation with extension from the socket).
- Damage to pulp and periodontal tissue.
- Long-term result: a tooth with non-vital pulp, but without destruction of bone tissue in the periapical area (Fig. 7).
Rice. 7. CT, visualization of tooth 23, MPR; trauma three years ago, obliteration of the middle and apical third of the root.
In recent years, dentistry as a science and applied branch of medicine has been actively developing, new technologies are being introduced into everyday practice, and world experience is being adopted. In this regard, it seems possible for us to recommend the Andreason classification and international terminology for use in our country. Below is a list and transcription of terms used in foreign literature when describing conditions associated with dental trauma.
- Fracture (fractura) - fracture.
- Subluxation - mobility without displacement, subluxation.
- Luxation is a dislocation of a tooth or displacement of a tooth fragment.
- Lateral luxation is a lateral displacement with fracture of the socket wall.
- Extrusion - extension from the hole.
- Intrusion - impacting, impacted dislocation (Fig. 8).
- Avulsion - “full luxation”, complete dislocation with tooth extraction.
- Contusion is a bruise of soft tissues.
- Abrasion - abrasion.
- Laceration (laceration) - rupture, dissection.
- Incision - incision, cut.
- Penetration - injury by a small object with its fixation in the tissues.
- Malformation is a developmental defect characterized by a change in shape and structure; violation of morphogenesis.
- Dilaceration - curvature of the root at a large angle or curvature of the crown relative to the root (Fig. 9).
- Inflamation - literally “fire”, inflammation, acute inflammation.
- Exacerbation - literally “outrage”, exacerbation of a chronic process.
Rice. 8. CT visualization of the coronal part of tooth 11 in a state of intrusion, an adult patient with a history of trauma to the primary incisor in childhood.
Rice. 9. CT visualization of rudiment 11, condition after trauma of primary incisors; after avulsion of the incisors, the tooth germ 11 develops in a state of dilaceration; the injury provoked the development of a follicular cyst from germ 11.
A dental therapist examines a patient with dental trauma. He also treats the patient, if necessary, involving a surgeon, orthodontist, or orthopedist. The examination consists of clarifying the victim’s complaints, medical history (questioning), determining the general condition of the patient and the condition of the periodontium in the area of the injured tooth, analyzing the data obtained, establishing a diagnosis and developing a treatment plan.
Until recently, radiodiagnosis (x-ray diagnostics) in dentistry was considered an additional research method, however, when examining injured teeth, this type of research has always been necessary and relevant. Therefore, with regard to dental trauma, we can say that radiodiagnostic testing is mandatory in all cases of trauma.
The maximum information about the condition and position of the injured tooth, as well as the degree of damage to the surrounding bone tissue, is provided by computed tomography (CT), performed on a specialized maxillofacial tomograph with cone beam collimation.
Research using spiral and sequential computed tomographs is extremely rarely used in dentistry, especially in pediatric practice, due to the high radiation exposure and low resolution of image receivers. However, cone beam CT scans with a single planar sensor are designed specifically for examining the maxillofacial region.
Devices of this class provide high image quality, and the radiation dose is only 30-60 microsieverts (0.03-0.06 mSv, which is 2-3 times less than, for example, with conventional radiography of the paranasal sinuses), therefore this method has no direct contraindications for use in pediatric dentistry.
If it is not possible to make a computed tomogram, it is necessary to perform polypositional intraoral radiography. Depending on the sector the tooth belongs to, intraoral photographs are taken in direct (orthoradial) and oblique (eccentric) projections.
It should not be forgotten that, firstly, the study is carried out in cases of severe pain, changes in the configuration of the tissues surrounding the tooth and, in many cases, contamination of the surrounding mucous membrane with blood.
Secondly, to avoid projection distortion when photographing single-rooted teeth, it is necessary to position the image receiver parallel to the vertical axis of the tooth being examined. In this regard, we recommend carrying out the most non-contact and apodactyl positioning with a parallel position of the tooth axis relative to the plane of the sensor or film (orthogonal projection).
When working with a radiovisiograph, this is easily done using a standard positioner. If film is used during the study, it must be fixed in a film-fixer or held by the edge of the cover with a mosquito-type clamp.
In case of combined trauma, panoramic tomography of the dentition (orthopantomography) is performed, however, in case of isolated damage to one or more teeth in the frontal region, this research method should be considered uninformative.
Initially, it is necessary to determine the quality of the radiograph: contrast, sharpness, projection distortions (lengthening, shortening of teeth). The image should be decrypted taking into account these data or a new image should be taken, avoiding previous mistakes.
An analysis of the shadow of the tooth should be carried out, paying attention to the outlines of the crown and root of the tooth, the presence of a cavity in the crown, a filling, and its defects (overhanging edges, loose fit to the walls of the cavity). When studying the image, the size, shape, location of the tooth cavity, the presence of a denticle or intracanal granuloma in it, the location and size of the canal mouths are revealed.
The condition of the root is determined from the radiograph: length, shape, contours, canal width, size of the apical foramen, which characterize the degree of root formation and reveal physiological or pathological root resorption. It is necessary to pay attention to the state of the space of the periodontal ligament and the closing hard plate of the alveolus (lamina dura), monitor its integrity, configuration and compliance with the anatomical shape.
It is necessary to evaluate the condition of the bone tissue surrounding the tooth, the outlines of the apexes of the interdental septa, their relationship with the enamel-cement border, integrity, extent, evaluate the configuration of the bone pattern, identify the presence of pathological changes and determine their nature. Radiation diagnostics are carried out immediately at the time of treatment, several months later, and also, in some cases, a day after the injury.
Repeated identical radiographs of the injured tooth, taken at various intervals, are necessary not only for dynamic monitoring of reparative processes, but also to clarify the diagnosis. This is due to the fact that immediately after the injury (several hours), if there is no significant mobility or change in the position of the coronal part of the tooth, the fracture line may not be visualized. Over time, the fragment shifts, associated with increased swelling of the surrounding tissues and mechanical impact on the crown during chewing, the gap between the fragments widens and becomes clearly visible on the image (Fig. 10).
Rice. 10. Intraoral photographs of tooth 21: a - an hour after the injury, b - a day later.
Despite the rapid development of technology and improvement of treatment methods, acute dental trauma still remains a pressing problem in dentistry. It is almost impossible to foresee or take any measures to prevent situations that provoke dental injury. In this regard, the prognosis in the treatment of OTD largely depends on a timely and correct diagnosis, on the basis of which the optimal treatment method will be selected.
Signs
The most common and obvious sign of a tooth fracture is pain, which in some cases can be very severe. Pain sensations increase noticeably at the moment of closing and opening the jaw. If we are talking about a minimal fracture (the enamel is damaged, but the pulp and dentin layer are kept healthy), the pain will be less noticeable compared to a tooth root fracture.
Fractures can be complete or incomplete. During the first, the pulp is opened, as a result of which various irritants can make the pain more severe. Complete fractures are considered to be a fracture of the entire root or its apex, as well as a fracture of the neck of the tooth. In case of an incomplete fracture, damage to dentin and enamel may occur.
Additional symptoms of tooth fractures may include loosening of teeth, problems with speech, bleeding gum tissue, and difficulty opening or closing the mouth.
Causes
The most common cause of a fracture is trauma. A sharp blow, a fall, or a car accident often lead to such damage.
Many patients break their teeth when chewing hard foods, and some deliberately chew on various inedible objects, which ultimately leads to damage.
The root may be damaged during dental treatment. Unprofessional cleaning and expansion of canals can cause injury.
Strong, healthy teeth are quite resistant to mechanical stress. Enamel cracks, insufficient mineralization, and caries significantly increase the risk of fracture even with minor impact.
Varieties
In addition to those mentioned above, there are the following types of fractures:
- Transverse. This is the least problematic option, especially if the pulp is not damaged. The choice of treatment method is determined taking into account the degree of the fracture. If only the crown is damaged, it can be increased. If the pulp is damaged, in most cases it must be removed, after which the tooth is restored based on the existing root. If, as a result of the fracture, only the root remains, the tooth is built up with pins.
- Longitudinal or vertical. In this case, it is impossible to restore the tooth with a pin, since the remnants of the root are not capable of serving as the basis for a crown or pin. If an element of the dentition is broken in half, it is very difficult to identify the problem. People often waste time, and the condition of the tissue quickly deteriorates, as a result of which the tooth is usually removed.
- Splintered and oblique. In such situations, the development of events occurs approximately the same as in the case of longitudinal fractures.
Crown fracture
This is one of the types of transverse fractures, it is quite easy to identify. The choice of treatment depends on the size of the chipped segment and the condition of the pulp. If the dentin is not damaged, but only part of the enamel is affected, a composite filling is the solution. In case of a fracture of the front tooth, extensions or veneers can be used.
If dentin is affected, doctors use special insulating pads. In cases where a tooth breaks in half and the pulp is damaged, it is removed and the canal is filled. Next, a pin can be installed followed by the use of a filling composite in order to restore the original shape.
A fracture of the neck of the tooth is also common. There are cases when the tooth wall breaks completely, but the pulp sac is not damaged. Typically, in such situations, specialists are in no hurry to get rid of the root, since it can become a good basis for a pin. In this case, in any case, the pulp is removed.
Prevention
Take regular care of your mouth, visit the dentist, and eat right. This will minimize the risk of damage.
Do not chew hard objects, get rid of such bad habits. At one point, your oral cavity may suffer. Do not eat excessively hard foods or dishes that may contain bones; eat them carefully.
Trust endodontic treatment only to an experienced, competent dentist. This will help avoid damage.
You can break a tooth through negligence. Try to avoid such life situations. The injury is very painful and the cost of recovery can be significant.
Root fracture
In the event of a tooth root fracture, a specialist analyzes its position to select the appropriate treatment. The fracture can occur near the neck, at the apex, in the middle part, or at the border of the upper and middle parts. In most cases, transverse fractures occur.
Diagnosis of such damage does not cause any difficulties. First of all, a person feels pain while chewing food and biting it. During palpation, mobility of the injured element of the dentition is observed. When percussing and closing the jaw, the patient experiences discomfort and pain. And if the fracture is located near the crown, the enamel may take on a pink tint. Radiography helps to clearly establish the number of cracks, as well as their position.
Enamel fracture (chip)
When the enamel is fractured, its surface layer usually breaks off. Patients do not complain of pain, they are concerned about cosmetic defects. Chipping most often occurs at the corner of the tooth; the sharp edges of the chip injure the mucous membranes of the oral cavity.
X-ray examination does not reveal any changes in the dental tissue; transillumination examination can reveal enamel cracks at the edges of the chip. When a chip is combined with a tooth bruise, pulp death is possible.
Treatment for an enamel fracture involves grinding off the sharp edges and applying fluoride varnish to the fracture plane to protect the tooth from caries. Chips are restored using artistic restoration - extension is carried out with composite materials. If the pulp dies, it must be removed followed by filling the root canals.
Treatment options
First of all, patients are prescribed an odontometric and x-ray examination. The information obtained helps determine the degree of fracture, the presence or absence of fragments, the condition of the pulp, as well as the number of fractures and their direction. If there is minimal damage, for example, a fracture of a front tooth with a small chip, its natural shape is restored using appropriate composite materials.
If oblique, comminuted or vertical fractures are found, in most cases the tooth must be removed, since its root is not capable of becoming a full-fledged basis for restoration with a pin. Usually the problem is solved by tooth extraction and further use of implantation.
If a tooth is broken at the root, it can also be restored. Otherwise, a metal-ceramic crown is used, the appearance of which is completely identical to the shape and color of the natural tooth.
If the pulp is damaged, it is usually removed. Then the canal is filled and the tooth is restored using a filling. But you must also make sure that its shape looks natural. Otherwise, closing the jaw may cause subsequent damage to the restored tooth. Another possible problem is the formation of an incorrect bite.
If a dead tooth is fractured at the root, implantation is used or a crown is installed. When a wisdom tooth is fractured, specialists usually remove them immediately. Limited access to these teeth makes them extremely difficult to fully restore.
The crown part of the front tooth is broken
If a front tooth is partially fractured, veneers or crowns can be used.
Veneers restore tooth function, protect dentin from external influences, and also the aesthetics of a smile. Treatment is only suitable for slightly damaged teeth. If the dental crown is severely damaged, the dentist will suggest installing a ceramic crown.
Crowns are placed on the remaining part of the tooth after grinding and preparing the surrounding area around the damaged tooth. If a significant part of the tooth has broken off, then to securely fix the crown it will be necessary to make a stump inlay, and in this case the tooth will have to be depulped (remove the nerve and fill the root canal).
The main stages of tooth restoration using a crown:
- Drawing up and agreeing on a treatment plan;
- Next, the doctor grinds the tooth down for a crown;
- Taking a silicone impression. The impression is sent to the dental laboratory. Based on the impression, the technicians reconstruct a plaster model of the teeth, and the technician will model the crown on it;
- When the crown is made, it is tried on and, if there is no discomfort, fixed on the stump.
To close the aesthetic defect, until the permanent crown is made, I install temporary plastic crowns on the patient, which can be made either in the laboratory or in the clinic.
Material for making dental crowns . Front teeth are a person’s calling card. When smiling, in conversation, every person involuntarily exposes his front teeth. Their beauty and health attract their interlocutor. This is why choosing the type of crown for teeth in the smile area is so important. The main types of permanent dental crowns are metal-ceramics, metal-free ceramics and ceramics with a zirconium dioxide frame. The most preferable material, from an aesthetic point of view, for the manufacture of dental crowns for the front teeth is metal-free ceramics e.max or feldspathic ceramics, also ceramics with a zirconium dioxide frame.
Alveolar ridge fractures
The appearance of such fractures occurs as a result of a direct blow, which affects several adjacent teeth at once. Since the upper jaw is in front, it is the one that suffers in most cases. This fracture can be determined by painful palpation, as well as the presence of damage to the mucous membranes. The process begins to move, and elements of the dentition may be broken or dislocated. Part of the jaw may be torn out or supported only by soft tissues.
Such a significant jaw injury is usually accompanied by dizziness, severe headaches, traumatic brain injury, and nausea. Using an x-ray, you can determine the location and direction of damage, as well as determine whether the broken part can be repaired. If it is viable, the specialist installs a splint that provides fixation of the bone for full fusion. In case of serious injuries, teeth that cannot be restored are removed, followed by fixation of the alveolar process.
If the injury is irreversible, the broken part is removed, since in the event of a rupture of the periosteum and adjacent soft tissues, the process usually cannot take root. In such situations, the damaged area is covered by the periosteum.
Diagnosis of tooth fracture
A fracture of the coronal part, while maintaining the integrity of the root, can be diagnosed by carefully examining the oral cavity, the tooth itself and the mucous membrane. After which the patient is given an x-ray, in which the fracture line can be clearly seen. On an x-ray, it looks like a thin cleared stripe. Electroodontometry will help determine how viable the pulp is.
Diagnosis of a fracture in the root part also begins with a visual examination. In this case, it is important to establish exactly where the root is and how mobile the tooth is. The doctor clarifies how severe the pain is, what its nature is, and what caused the injury. Next, you should also take an x-ray to create a proper treatment plan.
Tooth extraction after a fracture
It is necessary to remove a tooth only if it cannot be restored. If, after a fracture, an element of the dentition becomes loose, it is necessary to seek the help of a specialist as quickly as possible.
Tooth extraction is performed under anesthesia. Thanks to this, a person can completely relax and also get rid of pain. Usually everything happens very quickly, but in complex cases when a serious fracture has occurred, difficulties may arise. Sometimes the specialist has to cut the gum and pull out the remaining parts of the root, after which sutures are placed in this place. After some time they are removed. Depending on the specifics of a particular case, a specialist may recommend physical therapy and the installation of a dental implant.
Clinical manifestations of tooth fracture
Destruction of the crown without opening the pulp and with the root intact does not, in principle, bother patients with anything other than an unaesthetic appearance. Sometimes there may be pain when eating or drinking hot or cold things.
Chipping of the crown is often accompanied by hematomas, wounds and hemorrhage on the tongue and the inside of the cheeks. The sharp edges of a damaged tooth scratch delicate soft tissues. It is characterized by sharp throbbing pain and an instant reaction to stimuli. Such injuries are easy to notice visually, which is expressed as a small red dot.
You can find out whether the root is broken by trying to loosen the tooth in the socket. If it is mobile and you feel aching pain that intensifies when biting, then you should consult a dentist. The higher the level of fracture, the less mobile the tooth is.
Sometimes a broken tooth changes its color from white to pinkish. This is observed when the damage is localized in the apical part. However, if the vascular bundle has not been ruptured, then this sign may be absent.
We know how to cure a TOOTH FRACTURE
In the near future, a medical coordinator will contact you and advise you on the conditions and cost of treatment, select a doctor and make an appointment for you.
| Make an appointment | Or call us +375 29 699-03-03 +375 33 319-03-03 |